
Human emerging respiratory pathogens bulletin: Issue 94, October 2024

Download in PDF format
(609 KB, 5 pages)
Organization: Public Health Agency of Canada
Date published: 2024-11-12
Cat.: HP38-6E-PDF
ISBN: 2563-9420
Pub.: 230012
Monthly situational analysis of emerging respiratory diseases affecting humans (data to October 31, 2024).
In this bulletin
- Avian influenza updates
- Swine influenza updates
- Middle East respiratory syndrome coronavirus (MERS-CoV) update
| Novel influenzaFootnote 1 | Cumulative Case CountFootnote 2 | Deaths | Case Fatality Rate %Footnote 3 | Date of Last ReportFootnote 4 |
|---|---|---|---|---|
| Avian Influenza | ||||
| A(H1N2)Footnote 5 | 2 | 0 | 0% | January 2019 |
| A(H3N8) | 3 | 1 | 33% | March 2023 |
| A(H5NX)Footnote 6 | 8 | 0 | 0% | October 2024 |
| A(H5N1) | 944 | 470 | 50% | October 2024 |
| A(H5N2) | 1 | 1 | 100% | May 2024 |
| A(H5N6) | 93 | 57 | 61% | July 2024 |
| A(H5N8) | 7 | 0 | 0% | February 2021 |
| A(H7N4) | 1 | 0 | 0% | February 2018 |
| A(H7N9) | 1,568 | 615 | 39% | April 2019 |
| A(H9N2) | 134 | 2 | 1% | October 2024 |
| A(H10N3) | 3 | 0 | 0% | April 2024 |
| A(H10N5) | 1 | 1 | 100% | January 2024 |
| Swine Influenza | ||||
| A(H1N1)v | 50 | 2 | 4% | August 2024 |
| A(H1N2)v | 55 | 0 | 0% | August 2024 |
| A(H3NX)vFootnote 7 | 1 | 0 | 0% | August 2023 |
| A(H3N2)v | 451 | 1 | <1% | September 2024 |
| A(H1NX)vFootnote 8 | 1 | 1 | 100% | November 2021 |
| Eurasian avian-like A(H1N1)v | 11 | 0 | 0% | September 2023 |
| MERS-CoVFootnote 1 | ||||
| Global Case CountFootnote 9 | 2,614 | 943 | 36% | September 2024 |
| - Within Saudi ArabiaFootnote 10 | 2,205 | 863 | 39% | September 2024 |
|
||||
The Human Emerging Respiratory Pathogens (HERP) Bulletin is a monthly publication developed by the Public Health Agency of Canada (PHAC)'s Centre for Emerging and Respiratory Infections and Pandemic Preparedness (CERIPP). The HERP Bulletin serves as a mechanism for information sharing on summary surveillance indicators of global, including domestic, public health events affecting humans in the field of emerging respiratory pathogens. This includes pathogens such as novel influenzas (both avian and swine-origin), Middle East Respiratory Syndrome Coronavirus (MERS-CoV), and other ad-hoc emerging respiratory pathogens.
Monthly Highlights
Events in Canada
No human cases of emerging respiratory infection have been detected in Canada since the last detection in July 2024 (see HERP Bulletin no 91).
International Events
During the month of October 2024, the following human cases have been reported internationally (Figure 1):
- Twenty-five new human cases of avian influenza A(H5NX) (eighteen A(H5N1) and seven A(H5NX))
- One new human case of avian influenza A(H9N2)

Figure 1 : Descriptive text
- Eighteen (18) A(H5N1) cases were reported in the United States.
- One (1) A(H9N2) case was reported in China.
Note: Map was prepared by CERIPP using data from the latest WHO Event Information Site (EIS) postings. This map reflects data available through these publications as of October 31, 2024.
Avian influenza updates
Avian influenza A(H5N1)
Twenty-five new human cases of avian influenza A(H5NX) were reported in October 2024 from the US.
Sixteen human cases of avian influenza A(H5N1) were reported from California in October 2024. The cases involved dairy farm workers who were exposed to dairy cattle infected with A(H5N1). The cases were >18-years-old. All the cases experienced mild symptoms, including eye redness or discharge (conjunctivitis), and at least one case reported fever, cough, shortness of breath, and body aches. The cases were all treated according to US CDC guidelines and none were hospitalized. Genetic sequencing of 11 of these cases confirms that all are H5N1 viruses from clade 2.3.4.4b. The whole genome sequencing of viruses detected in four cases has confirmed they are all xB3.13 genotype, which are closely related to viruses detected in dairy cattle in the US.
A total of two human cases of avian influenza A(H5N1) and seven human cases of avian influenza A(H5NX) were reported in Washington State. Prior to illness onset, all nine cases had exposure to A(H5N1) infected poultry and at least two of these cases are agricultural workers in Franklin County who were performing disposal and depopulation operations at a poultry facility. Both of the confirmed A(H5N1) cases had conjunctivitis, and one had cough and muscle aches. Both A(H5N1) cases were offered oseltamivir, and they were not hospitalized.
Serologic testing was performed for the Missouri case reported in September 2024 (see HERP Bulletin no 93) and six close contacts. Serologic test results for the case and one household contact showed evidence of an antibody immune response to A(H5) in only one assay, but not on other serologic assays that are used to detect infection. Serologic test results for five healthcare worker close contacts showed no signs of previous A(H5N1) infection. The results from these serologic tests and the US CDC's investigation suggest that human-to-human transmission did not occur.
In 2024, 44 human cases of avian influenza A(H5N1) have been detected worldwide, from Australia (1), Cambodia (10), China (1), the United States (31), and Vietnam (1). This case count does not include the seven A(H5NX) human cases in the US that were reported in October 2024 nor the one A(H5NX) human case in the US where the US CDC was not able to determine the subtype of the neuraminidase (NA). Since the start of the ongoing A(H5N1) worldwide outbreak in poultry and other animals in December 2021, 63 human cases of A(H5N1) have been reported worldwide (2022: n=6, 2023: n=13, 2024: n=44) in Australia (1), Cambodia (16), Chile (1), China (3), Ecuador (1), Spain (2), United Kingdom (5), United States (32), and Vietnam (2) (Figure 2). Of these cases, 34 of the viruses belong to the same strain of A(H5N1) that is associated with the current global outbreak in animals (clade 2.3.4.4b), 12 cases were infected with viruses that belonged to a different strain of A(H5N1) (clade 2.3.2.1c), and one is from clade 2.3.2.1a. One case is tentatively from clade 2.3.4.4b and the clade details of five cases from Cambodia, the travel-related case from China, and nine cases from the US are unknown.
Since the emergence of A(H5N1) in humans in 1997, 944 human cases of A(H5N1) have been reported globally, with a CFR of 50% (Figure 3). In Canada, A(H5N1) detections associated with the current 2021-2024 A(H5N1) clade 2.3.4.4b epizootic have been reported in domestic, backyard, and wild bird populations, as well as other animal species. HPAI A(H5N1) has not been detected in dairy cattle, other livestock in Canada, or in raw milk. No domestically acquired human A(H5N1) infections have ever been reported in Canada; however, in 2014, Canada (Alberta) reported a single fatal case of A(H5N1) in a resident returning from travel in China.
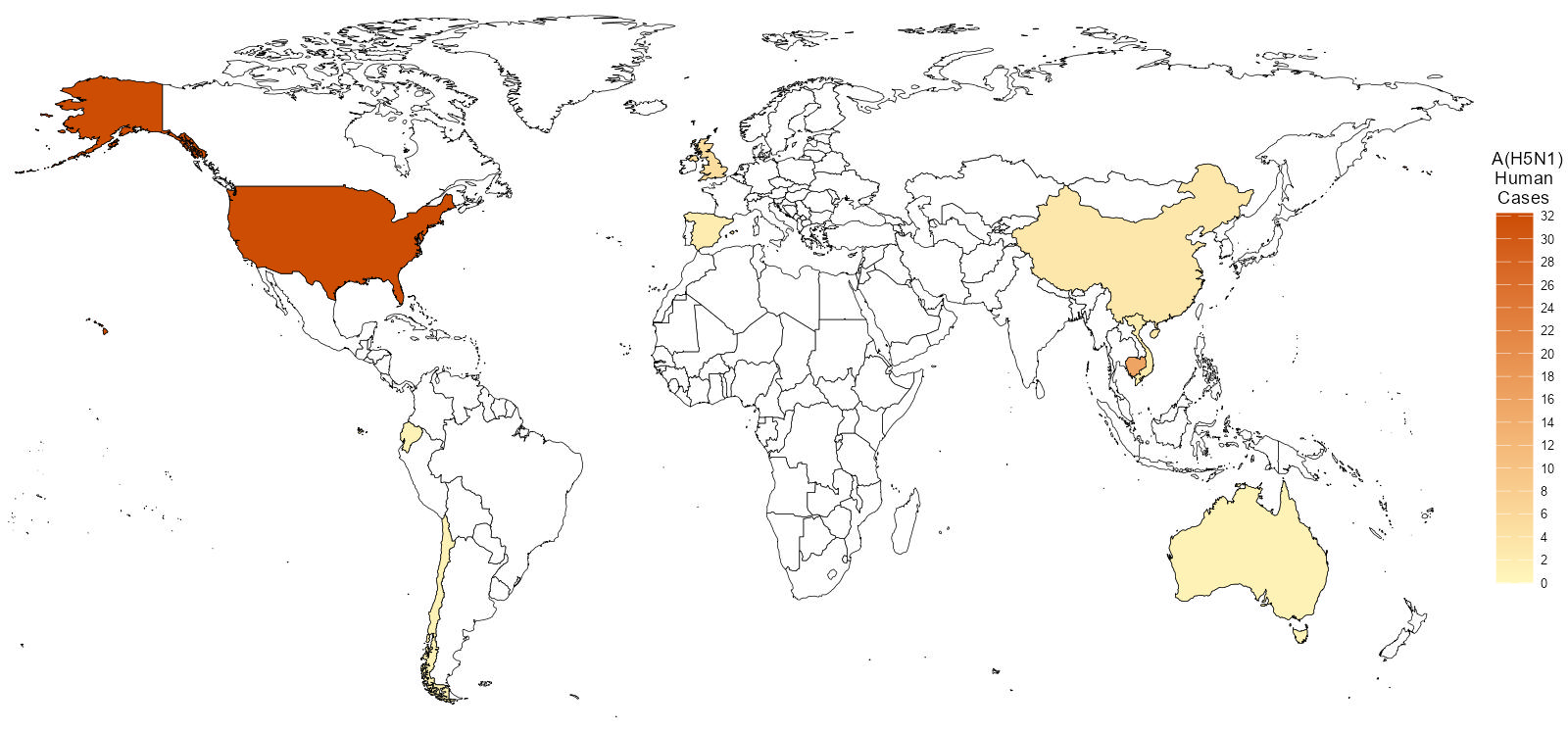
Figure 2 : Descriptive text
- One (1) case was reported out of Australia.
- Sixteen (16) cases were reported out of Cambodia.
- One (1) case was reported out of Chile.
- Three (3) cases were reported out of China.
- One (1) case was reported out of Ecuador.
- Two (2) cases were reported out of Spain.
- Five (5) cases were reported out of the United Kingdom.
- Thirty-two (32) cases were reported out of the United States of America.
- Two (2) cases were reported out of Vietnam.
Note: Map was prepared by CERIPP using data from the WHO EIS postings, the US CDC's Health Alert Network (HAN), and WHO cumulative case counts. This map reflects data available as of October 31, 2024.
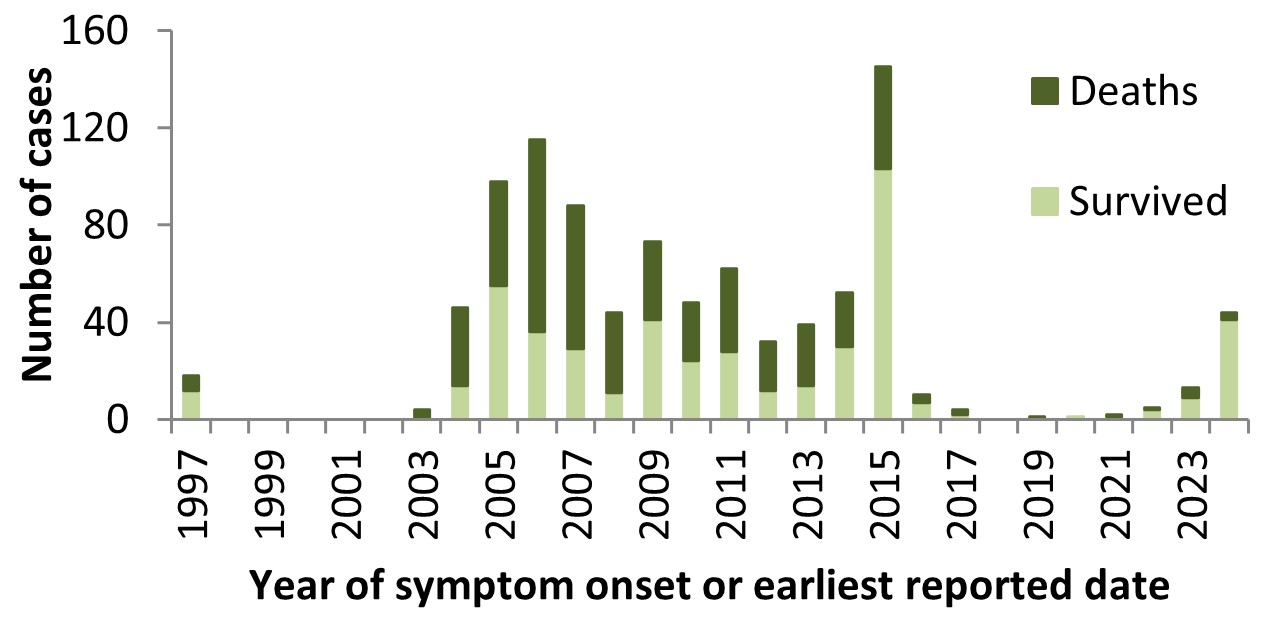
Figure 3 : Descriptive text
| Number of Cases | Deaths | Survived | |
|---|---|---|---|
| 1997 | 18 | 6 | 12 |
| 1998 | 0 | 0 | 0 |
| 1999 | 0 | 0 | 0 |
| 2000 | 0 | 0 | 0 |
| 2001 | 0 | 0 | 0 |
| 2002 | 0 | 0 | 0 |
| 2003 | 4 | 4 | 0 |
| 2004 | 46 | 32 | 14 |
| 2005 | 98 | 43 | 55 |
| 2006 | 115 | 79 | 36 |
| 2007 | 88 | 59 | 29 |
| 2008 | 44 | 33 | 11 |
| 2009 | 73 | 32 | 41 |
| 2010 | 48 | 24 | 24 |
| 2011 | 62 | 34 | 28 |
| 2012 | 32 | 20 | 12 |
| 2013 | 39 | 25 | 14 |
| 2014 | 52 | 22 | 30 |
| 2015 | 145 | 42 | 103 |
| 2016 | 10 | 3 | 7 |
| 2017 | 4 | 2 | 2 |
| 2018 | 0 | 0 | 0 |
| 2019 | 1 | 1 | 0 |
| 2020 | 1 | 0 | 1 |
| 2021 | 2 | 1 | 1 |
| 2022 | 5 | 1 | 4 |
| 2023 | 13 | 4 | 9 |
| 2024 | 44 | 3 | 41 |
Note: Graph was prepared by CERIPP using data from the WHO EIS postings, the US CDC's Health Alert Network (HAN), and WHO cumulative case counts. This graph reflects data available as of October 31, 2024.
Avian influenza A(H5N2)
The most recent human case of avian influenza A(H5N2) was reported in May 2024 from Mexico.
This was the first ever detected human case of A(H5N2). Since only one human case of A(H5N2) has been reported to date and the availability of clinical information is limited, the full spectrum of disease is unknown.
Avian influenza A(H5N6)
The most recent human case of avian influenza A(H5N6) was reported in July 2024 from China.
Since January 2021, 67 cases of avian influenza A(H5N6) have been reported globally (2021: n=32, 2022: n=25, 2023: n=5, 2024: n=4) (Figure 4); all but one case (2021, Lao PDR) were reported in China. Since the emergence of this virus in 2014, a total of 93 laboratory-confirmed human cases of avian influenza A(H5N6), including at least 57 deaths, have been reported globally (CFR: 61%). No cases have been reported in Canada.
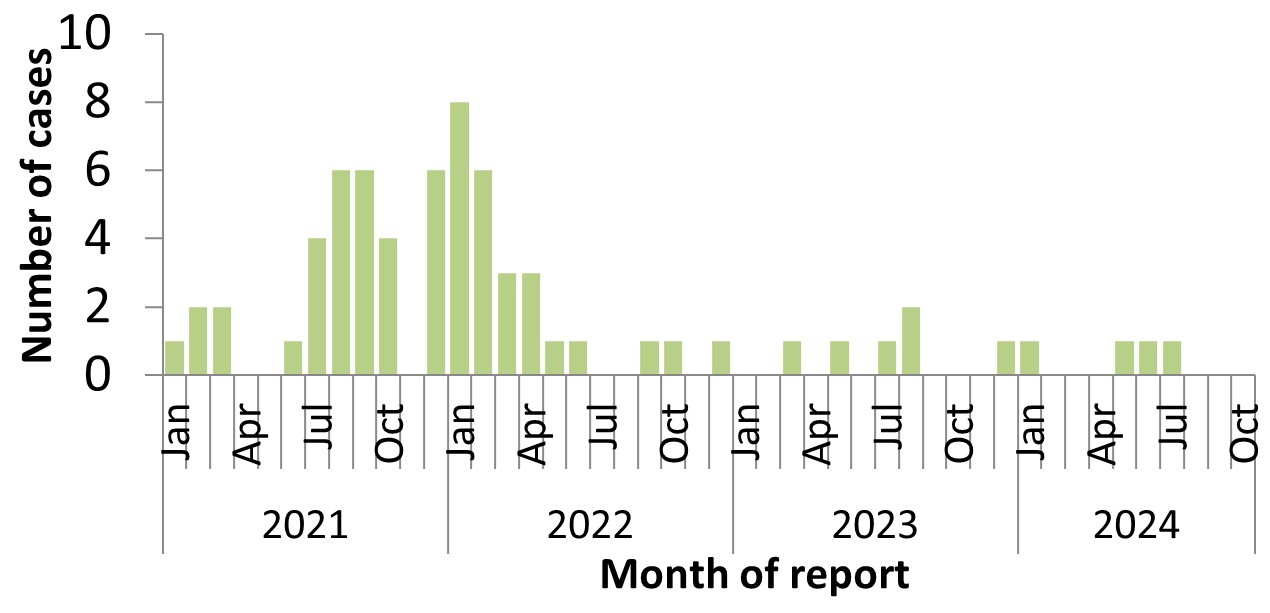
Figure 4 : Descriptive text
| Month | Cases | |
|---|---|---|
| 2021 | Jan | 1 |
| Feb | 2 | |
| Mar | 2 | |
| Apr | 0 | |
| May | 0 | |
| June | 1 | |
| July | 4 | |
| Aug | 6 | |
| Sep | 6 | |
| Oct | 4 | |
| Nov | 0 | |
| Dec | 6 | |
| 2022 | Jan | 8 |
| Feb | 6 | |
| Mar | 3 | |
| Apr | 3 | |
| May | 1 | |
| June | 1 | |
| July | 0 | |
| August | 0 | |
| Sep | 1 | |
| Oct | 1 | |
| Nov | 0 | |
| Dec | 1 | |
| 2023 | Jan | 0 |
| Feb | 0 | |
| Mar | 1 | |
| Apr | 0 | |
| May | 1 | |
| June | 0 | |
| July | 1 | |
| August | 2 | |
| Sep | 0 | |
| Oct | 0 | |
| Nov | 0 | |
| Dec | 1 | |
| 2024 | Jan | 1 |
| Feb | 0 | |
| Mar | 0 | |
| Apr | 0 | |
| May | 1 | |
| June | 1 | |
| July | 1 | |
| August | 0 | |
| Sep | 0 | |
| Oct | 0 |
Note: Graph was prepared by CERIPP using data from the WHO EIS postings and the Hong Kong Centre for Health Protection (CHP) press releases. This graph reflects data available as of October 31, 2024.
Avian influenza A(H9N2)
One new human case of avian influenza A(H9N2) was reported in October 2024 from China.
The case was a 3-year-old male from Chongqing municipality. His illness onset date was September 4, 2024, and on September 5, 2024, he was brought to the hospital with fever and rhinorrhea. The case experienced mild symptoms, was not hospitalized, and has recovered. Prior to illness onset, the case had played near a live poultry stall at a nearby market. A total of three close contacts were identified, screened, and monitored. None of them had any respiratory symptoms at the time of reporting. Samples from close contacts tested negative for influenza, and no family cluster was detected. Environmental samples from the live stalls in the market tested positive for H9, including one sample from the live poultry stall near where the case previously played.
In 2024, 12 human cases of avian influenza A(H9N2) have been reported worldwide, from China (9), India (1), Vietnam (1), and Ghana (1). In 2023, a total of 15 human cases of avian influenza A(H9N2) were reported globally, all in China. Since the emergence of avian influenza A(H9N2) in the human population in 1998, 134 cases have been reported worldwide, with a CFR of approximately 1%. No cases have been reported in Canada.
Avian influenza A(H10N3)
The most recent human case of avian influenza A(H10N3) was reported in April 2024 from China.
In 2024, one human case of avian influenza A(H10N3) has been reported worldwide. Since the emergence of avian influenza A(H10N3) in humans in 2021, three human cases have been reported, all from China, with a CFR of 0%. However, with only three human cases reported to date, the full spectrum of disease is highly uncertain. No cases have been reported in Canada.
Swine influenza updates
Swine origin influenza A(H1N1)v
The most recent human cases of swine origin influenza A(H1N1)v were reported in August 2024 from the US (1) and Vietnam (1).
In 2024, four human cases of swine origin influenza A(H1N1)v have been detected worldwide. There have been five human A(H1N1)v cases reported worldwide in 2023 in Brazil (1), China (2), Spain (1) and Switzerland (1). A total of 50 human cases of A(H1N1)v have been reported globally since 2005, with a 4% CFR. Two A(H1N1)v detections have been reported in Canadian residents since reporting began in 2005, with the first case reported in Ontario in September 2012 and the second case reported in Manitoba in April 2021 (see HERP Bulletin no 52).
Swine origin influenza A(H1N2)v
The most recent human case of swine origin influenza A(H1N2)v was reported in August 2024 from the US.
In 2024, three human cases of swine origin influenza A(H1N2)v were detected worldwide, all in the United States. In 2023, four human swine origin influenza A(H1N2)v cases were reported worldwide in Taiwan (1), the UK (1), and the United States (2). A total of 55 human cases of swine origin influenza A(H1N2)v have been reported globally since 2005, with a 0% CFR. Three swine origin influenza A(H1N2)v detections have been reported in Canadian residents since reporting began in 2005. The first case was reported in Alberta in October 2020 (see HERP Bulletin no 46), the second case was reported in Manitoba in April 2021 (see HERP Bulletin no 52) and the latest case in Canada was reported in November 2021 in Manitoba (see HERP Bulletin no 59).
Swine origin influenza A(H3N2/H3NX)v
The most recent human cases of swine origin influenza A(H3N2)v were reported in September 2024 from the US.
To date, five human cases of swine origin influenza A(H3N2)v have been reported worldwide in 2024, from Canada (1) and the United States (4). Excluding the reported case of A(H3NX)v in the United States (1), no cases of swine origin influenza A(H3N2)v were detected in 2023. Globally, 451 swine origin influenza A(H3N2)v cases have been reported since 2005, with <1% CFR. Four human cases of swine origin influenza A(H3N2)v have been reported in Canada since 2005. The first case of A(H3N2)v in Canada was reported in Ontario in 2005. This was followed by a second case in Ontario in 2016, a third case in Manitoba in June 2021 (see HERP Bulletin no 54), and a fourth case in Saskatchewan in July 2024 (see HERP Bulletin no 91).
Middle East respiratory syndrome coronavirus (MERS-CoV) update
The most recent human case of MERS-CoV was reported in September 2024 from the Kingdom of Saudi Arabia (KSA).
To date, six new human cases of MERS-CoV have been reported in 2024, all from Saudi Arabia. In 2023, ten cases of MERS-CoV were reported in Oman (1), Saudi Arabia (8), and the United Arab Emirates (1). According to the WHO, 2,614 laboratory-confirmed cases of MERS-CoV, including 943 deaths, have been reported globally since reporting began in 2012 (CFR: 36%) (Figure 5). No cases have ever been reported in Canada.
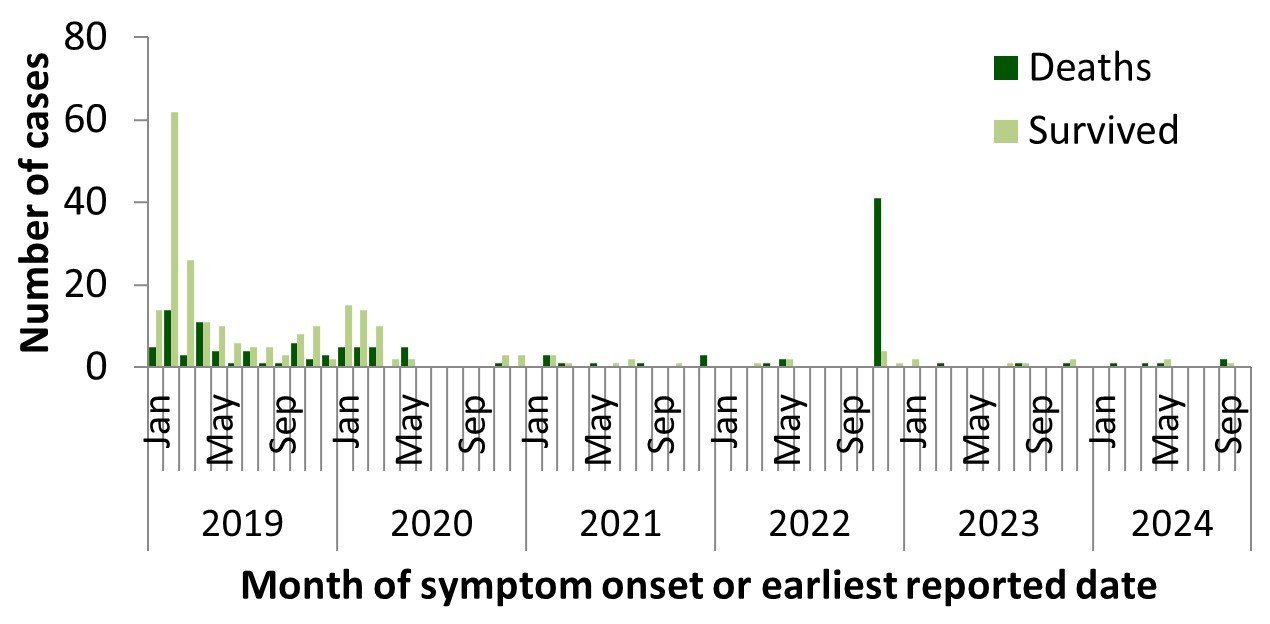
Figure 5 : Descriptive text
| Deaths | Survived | ||
|---|---|---|---|
| 2019 | Jan | 5 | 14 |
| Feb | 14 | 62 | |
| Mar | 3 | 26 | |
| Apr | 11 | 11 | |
| May | 4 | 10 | |
| June | 1 | 6 | |
| July | 4 | 5 | |
| Aug | 1 | 5 | |
| Sep | 1 | 3 | |
| Oct | 6 | 8 | |
| Nov | 2 | 10 | |
| Dec | 3 | 2 | |
| 2020 | Jan | 5 | 15 |
| Feb | 5 | 14 | |
| Mar | 5 | 10 | |
| Apr | 0 | 2 | |
| May | 5 | 2 | |
| June | 0 | 0 | |
| July | 0 | 0 | |
| Aug | 0 | 0 | |
| Sep | 0 | 0 | |
| Oct | 0 | 0 | |
| Nov | 1 | 3 | |
| Dec | 0 | 3 | |
| 2021 | Jan | 0 | 0 |
| Feb | 3 | 3 | |
| Mar | 1 | 1 | |
| Apr | 0 | 0 | |
| May | 1 | 0 | |
| June | 0 | 1 | |
| July | 0 | 2 | |
| Aug | 1 | 0 | |
| Sep | 0 | 0 | |
| Oct | 0 | 1 | |
| Nov | 0 | 0 | |
| Dec | 3 | 0 | |
| 2022 | Jan | 0 | 0 |
| Feb | 0 | 0 | |
| Mar | 0 | 1 | |
| Apr | 1 | 0 | |
| May | 2 | 2 | |
| June | 0 | 0 | |
| July | 0 | 0 | |
| Aug | 0 | 0 | |
| Sep | 0 | 0 | |
| Oct | 0 | 0 | |
| Nov | 41 | 4 | |
| Dec | 0 | 1 | |
| 2023 | Jan | 0 | 2 |
| Feb | 0 | 0 | |
| Mar | 1 | 1 | |
| Apr | 0 | 0 | |
| May | 0 | 0 | |
| June | 0 | 0 | |
| July | 0 | 1 | |
| Aug | 2 | 1 | |
| Sep | 0 | 0 | |
| Oct | 0 | 0 | |
| Nov | 1 | 2 | |
| Dec | 0 | 0 | |
| 2024 | Jan | 0 | 0 |
| Feb | 1 | 0 | |
| Mar | 0 | 0 | |
| Apr | 1 | 0 | |
| May | 1 | 2 | |
| June | 0 | 0 | |
| July | 0 | 0 | |
| Aug | 0 | 0 | |
| Sep | 2 | 1 | |
| Oct | 0 | 0 |
Note: Graph was prepared by CERIPP using data from the WHO Disease Outbreak News (DON) and Saudi Arabia's Ministry of Health. This graph reflects data available as of October 31, 2024. The data integrates CERIPP real-time reporting with WHO DON retrospective reporting of MERS-CoV cases and deaths. In November 2022, the WHO published a DON article that updated their counts with retrospective cases and deaths, which resulted in an increase of an additional 5 cases and 41 deaths compared to their previous MERS-CoV-related DON. In August 2023, the WHO published a DON article with case information for three retrospective MERS-CoV cases and two deaths. These three cases and one death were already reflected in the cumulative case count of the DON article published in July 2023, as well as the case totals published in HERP Bulletin no 79. In May 2024, the WHO published a DON article with case information for one single, fatal case of MERS-CoV. This fatal case was already reflected in the case totals published in HERP Bulletin no 88.
Page details
- Date modified: