
Human echinococcosis incidence in Canada, 2000–2020

 Download this article as a PDF (262 KB)
Download this article as a PDF (262 KB)Published by: The Public Health Agency of Canada
Issue: CCDR Volume 50-9, September 2024: Health Risk Assessment
Date published: September 2024
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 50-9, September 2024: Health Risk Assessment
Surveillance
Human echinococcosis incidence in Canada: A retrospective descriptive study using administrative hospital and ambulatory visit data, 2000–2020
Ayisha Khalid1,2, Pia K Muchaal1, Danielle A Julien1
Affiliations
- 1 Public Health Agency of Canada, Ottawa, ON
- 2 Dalla Lana School of Public Health, University of Toronto, Toronto, ON
Correspondence
Suggested citation
Khalid A, Muchaal PK, Julien DA. Human echinococcosis incidence in Canada: A retrospective descriptive study using administrative hospital and ambulatory visit data, 2000–2020. Can Commun Dis Rep 2024;50(9):305–11. https://doi.org/10.14745/ccdr.v50i09a03
Keywords: echinococcosis, incidence, administrative data, Canada
Abstract
Background: Echinococcosis is a zoonotic disease caused by the ingestion of tapeworm eggs shed by canids. The potential recent establishment of a more virulent European-type strain may be impacting human echinococcosis in Canada, yet information is limited.
Objective: Administrative hospital and ambulatory visit data were used to provide a baseline of human echinococcosis cases in Canada between 2000–2020.
Methods: Canadian Institute of Health Information's Discharge Abstract Database, Hospital Morbidity Database and National Ambulatory Care Reporting System were combined to identify cases. Risk ratios (RR) by demographic factors and cumulative incidences (CIN) over place and time were calculated.
Results: A total of 806 echinococcosis cases were identified in Canada between 2000–2020, for a mean annual CIN of 1.3 cases per million population. Over the two decades, the mean annual CIN of cases increased nationally (1.3–1.4 cases per million), in the Northwest Territories (6.3–9.1 cases per million), in Alberta (1.5–2.4 cases per million) and in the Atlantic provinces (0.2–0.6 cases per million). Those from the Territories had the highest risk of echinococcosis (RR 17.1; 95% confidence interval: 8.7–33.7).
Conclusion: Though explanations are multifactorial, the new European-type strain may have a role in the small absolute increase in echinococcosis CIN in Canada observed over the study period. The CIN is likely underestimated and the validity of administrative data for analyzing zoonoses warrants investigation. Though this study contributes important awareness and a baseline, improved data are needed to clarify the effects of the new strain and inform public health response.
Introduction
Echinococcosis is a rare zoonotic disease caused by infection with larval Echinococcus tapewormsFootnote 1. Tapeworm eggs are excreted in the feces of infected canids and can be ingested by humans through contaminated food, water or soil, or from close contact with infected animalsFootnote 1. Compared to the general population, those who have frequent contact with canids, such as dog owners, can face increased risk of echinococcosisFootnote 2. Some Indigenous Peoples in Canada, Alaska, Russia and Siberia north of the Arctic Circle who practise traditional cultural activities, such as using sled dogs, hunting, fishing and gathering, may also face increased riskFootnote 3Footnote 4Footnote 5. In isolated areas, use of untreated surface water as a potable water source and inaccessible medical services can compound risk and contribute to more severe health outcomesFootnote 5.
Echinococcosis in humans occurs in two major forms. Cystic echinococcosis (CE), caused by Echinococcus granulosus, leads to hydatid cysts in organs, often the liver and lungs, that can impair physiological functionFootnote 1. Alveolar echinococcosis (AE), caused by Echinococcus multilocularis, produces a tumour-like polycystic mass in organs, most often in the liver, that can infiltrate adjacent organs and tissues to produce distant metastasesFootnote 1. Treatment generally requires surgical removal or chemotherapyFootnote 1. Echinococcosis is frequently under or misdiagnosed because the disease is rare, awareness is limited, both AE and CE have long incubation periods ranging 5–15 years and up to 60% of cases are asymptomaticFootnote 1.
While both AE and CE have been reported in Canada, AE was historically limited to the North American E. multilocularis strain and found almost exclusively in wildlifeFootnote 6. In 2009, a new E. multilocularis strain more closely related to European strains was detected in a dog from British Columbia with no travel history outside of the provinceFootnote 7. Local canid transmission was identified thereafter in British Columbia as well as Alberta, Manitoba and OntarioFootnote 8Footnote 10Footnote 11. The first human case of AE with the European-type E. multilocularis strain was confirmed in Alberta in 2013Footnote 12. Of six subsequent human cases in Alberta, molecular typing was available for five, all indicating the presence of the European-type strainFootnote 13.
European E. multilocularis strains have greater virulence and zoonotic potential than North American strainsFootnote 8. Due to the potential establishment of the European-type strain in animal hosts, climate change, urbanization and anthropogenic activities, human AE is considered an emerging disease threat in CanadaFootnote 4Footnote 8. Yet, knowledge about human echinococcosis in the country is limited. While AE is a provincially notifiable disease in Alberta, Ontario, Nunavut and the Northwest Territories, it is currently not nationally notifiableFootnote 14.
Absence of information on echinococcosis among people in Canada, exacerbated by limited awareness and underdiagnosis, as well as increasing evidence of emergence due to the detection of a more virulent strain, necessitates the use of alternative nationwide data sources to describe echinococcosis. This study leveraged administrative hospital and ambulatory visit data to provide a baseline for human echinococcosis in Canada between 2000–2020, relevant for increasing awareness and informing public health guidelines. Risk ratios (RRs) by demographic factors and incidences over place and time of echinococcosis cases were estimated. The authors hypothesized a higher incidence in 2011–2020 than 2000–2010, especially in isolated northern areas, due to the European-type E. multilocularis strain detected in 2009.
Methods
Data sources
To identify echinococcosis cases, three Canadian Institute for Health Information (CIHI) databases were combined: the Discharge Abstract Database (DAD), Hospital Morbidity Database (HMDB) and National Ambulatory Care Reporting System (NACRS). These databases collect data on an annual basis corresponding to the fiscal year (April 1 of one year to March 31 of the following year)Footnote 15. The DAD and HMDB databases similarly capture national administrative, clinical and basic demographic information on hospital inpatient events, however, the DAD does not include data from QuébecFootnote 15. The NACRS contains complete or partial data on hospital-based and community-based ambulatory care from Alberta, British Columbia, Manitoba, Nova Scotia, Ontario, Prince Edward Island, Québec, Saskatchewan and YukonFootnote 15.
Eligibility criteria
Diagnoses in CIHI databases use the ninth or tenth revision of the World Health Organization's International Classification of Diseases (ICD-9 and ICD-10)Footnote 16Footnote 17. Cases were defined as patients visiting hospital or ambulatory care for whom the main responsible diagnosis or one of the first five discharge diagnoses was echinococcosis (ICD-9 codes 122.0 to 122.9; ICD-10 codes B67.0 to B67.9).
To derive the echinococcosis cases dataset, the available DAD, HMDB and NACRS data were first merged. Records of cases in years with incomplete data due to collection on a fiscal year basis were removed. Then, duplicates and records describing readmissions for echinococcosis for the same case were removed to align with the goal of estimating incidence. Specifically, the first chronological record was retained, regardless of which database it came from and subsequent records were excluded. The CIHI databases contain encrypted health card numbers that were used to find records for the same case. The SAS Enterprise Guide® 7.1 software for Microsoft Windows was used to merge data.
Data analysis
Descriptive analyses were used to characterize echinococcosis cases by infecting Echinococcus species, sex, age group and region and province/territory (P/T) of health card issuance. Bivariate analyses were used to determine the RR, with 95% confidence intervals (CI), of echinococcosis by sex, age group, region and P/T. Québec was excluded from RR calculations to avoid skewed comparisons, as data from the province were only available from the HMDB for the first half of the study period (2000–2010). Population estimates from Statistics Canada's 2011 Census of Population were used as denominators to compute RRsFootnote 18.
The cumulative incidence (CIN) of echinococcosis cases over 2000–2020 at the national, regional and P/T levels was calculated using annual population estimates (fourth quarter) from Statistics Canada as denominatorsFootnote 19. The mean annual CIN was calculated by taking an average of the yearly CIN of echinococcosis cases. Québec was excluded from CIN calculations. Data were analyzed using R Statistical Software (v4.1.1; R Core Team 2021) and QGIS Geographic Information System 3.8 was used to map CIN.
Results
Characteristics and risk ratios
The final dataset comprised 806 records of incident echinococcosis cases in Canada between 2000–2020 (Figure 1). The demographic characteristics of cases and RRs are presented in Table 1. Of the 806 cases, most were unspecified (n=669; 82.3%), followed by E. granulosus (n=111; 13.7%) and E. multilocularis (n=33; 4.1%). The largest proportion of cases (n=371; 46.0%) were from Ontario. Females comprised over half of cases (n=501; 62.2%) and were at 1.6 (95% CI: 1.4–1.8) times higher risk of echinococcosis compared to males. While most cases were aged 35–54 years (n=265; 32.9%), those over 75 years of age had the highest risk, at 5.6 (95% CI: 3.9–8.0) times higher than those aged 0–14 years.

Figure 1 - Text description
Records of echinococcosis cases were identified from CIHI databases (n=1,539), including DAD 1999–2000 to 2020–2021 (n=820), HMDB 1999–2000 to 2010–2011 (n=231) and NACRS 2002–2003 to 2020–2021 (n=488). Incomplete years were removed (n=108), including DAD 1999 and 2021, HMDB 1999 and 2011 and NACRS 2002 and 2021. There were n=1,431 records remaining after incomplete years were removed. Duplicates and re-admissions were then removed (n=625). Final records of incident echinococcosis cases (n=806) thus included DAD 2000–2020, HMDB 2000–2010 and NACRS 2003–2020.
Abbreviations: CIHI, Canadian Institute for Health Information; DAD, Discharge Abstract Database; HMDB, Hospital Morbidity Database; NACRS, National Ambulatory Care Reporting System
| Characteristics | Echinococcosis cases | |
|---|---|---|
| n (%) | Risk ratios (95% CI) |
|
| Echinococcus speciesFootnote b | ||
| E. multilocularis | 33 (4.1) | N/A |
| E. granulosus | 111 (13.7) | N/A |
| Unspecified | 669 (82.3) | N/A |
| Sex | ||
| Male | 305 (37.8) | 1.0 |
| Female | 501 (62.2) | 1.6 (1.4–1.8) |
| Age group | ||
| 0–14 years | 42 (5.2) | 1.0 |
| 15–34 years | 193 (23.9) | 3.0 (2.1–4.1) |
| 35–54 years | 265 (32.9) | 3.6 (2.6–5.0) |
| 55–74 years | 211 (26.2) | 4.0 (2.9–5.6) |
| ≥75 years | 95 (11.8) | 5.6 (3.9–8.0) |
| Geography | ||
| Atlantic region | 19 (2.4) | 1.0 |
| Prince Edward Island | 1 (0.1) | 1.0 |
| New Brunswick | 7 (0.9) | 1.3 (0.2–10.3) |
| Newfoundland and Labrador | 5 (0.6) | 1.3 (0.2–11.3) |
| Nova Scotia | 6 (0.7) | 0.9 (0.1–7.4) |
| Eastern region | 436 (54.1) | 3.5 (2.2–5.6)Footnote c |
| Ontario | 371 (46.0) | 3.9 (0.6–27.9) |
| Québec | 65 (8.1) | N/AFootnote c |
| Western region | 336 (41.7) | 4.0 (2.5–6.4) |
| Alberta | 155 (19.2) | 5.8 (0.8–41.3) |
| British Columbia | 102 (12.7) | 3.2 (0.4–22.6) |
| Manitoba | 37 (4.6) | 4.2 (0.6–30.3) |
| Saskatchewan | 42 (5.2) | 5.5 (0.8–40.1) |
| Territories region | 15 (1.9) | 17.1 (8.7–33.7) |
| Northwest Territories | 7 (0.9) | 22.9 (2.8–186.4) |
| Nunavut | 4 (0.5) | 17.0 (1.9–152.4) |
| Yukon | 4 (0.5) | 16.0 (1.8–143.4) |
Abbreviations: CI, confidence interval; E., Echinococcus; N/A, not applicable Footnotes
|
||
Cases with a health card issued from the Territories region (Northwest Territories, Nunavut and Yukon) had a much higher risk of echinococcosis (RR 17.1; 95% CI: 8.7–33.7) compared to the Atlantic region (New Brunswick, Newfoundland and Labrador, Nova Scotia and Prince Edward Island). Cases from the Northwest Territories had the highest risk of echinococcosis in the country, at 22.9 (95% CI: 2.8–186.4) times that of Prince Edward Island. Among provinces, cases from the Western region (Alberta, British Columbia, Manitoba and Saskatchewan) (RR 4.0; 95% CI: 2.5–6.4), compared to the Atlantic region, had the highest risk of echinococcosis.
Cumulative incidence
As shown in Table 2, the mean annual CIN of echinococcosis cases in Canada between 2000–2020 was 1.3 cases per million population. There was a slight absolute increase over the two decades nationally, from 1.3 cases per million between 2000–2010 to 1.4 cases per million between 2011–2020. The mean annual CIN of cases diagnosed as E. multilocularis increased very slightly over the two decades (0.05–0.06 cases per million), while cases diagnosed as E. granulosus decreased very slightly (0.19–0.18 cases per million). Detailed count and CIN by Echinococcus species, geography and year is provided in the Appendix as Supplemental material.
| Geography | Mean annual CIN (per million population) | ||
|---|---|---|---|
| Overall (2000–2020) |
First decade (2000–2010) |
Second decade (2011–2020) |
|
| National | 1.3 | 1.3 | 1.4 |
| E. multilocularis | 0.06 | 0.05 | 0.06 |
| E. granulosus | 0.20 | 0.19 | 0.18 |
| Unspecified | 1.1 | 1.1 | 1.1 |
| Atlantic region | 0.4 | 0.2 | 0.6 |
| New Brunswick | 0.4 | 0.4 | 0.5 |
| Newfoundland and Labrador | 0.5 | 0.4 | 0.6 |
| Nova Scotia | 0.3 | 0.1 | 0.5 |
| Prince Edward Island | 0.3 | 0 | 0.6 |
| Eastern region | 1.3Footnote b | 1.4Footnote b | 1.3Footnote b |
| Ontario | 1.3 | 1.4 | 1.3 |
| Québec | N/AFootnote b | N/AFootnote b | N/AFootnote b |
| Western region | 1.6 | 1.6 | 1.6 |
| Manitoba | 1.4 | 1.4 | 1.5 |
| Saskatchewan | 1.9 | 2.0 | 1.8 |
| Alberta | 1.9 | 1.5 | 2.4 |
| British Columbia | 1.1 | 1.4 | 0.8 |
| Territories region | 6.2 | 6.8 | 5.6 |
| Northwest Territories | 7.6 | 6.3 | 9.1 |
| Nunavut | 5.8 | 8.6 | 2.6 |
| Yukon | 5.2 | 5.3 | 5.1 |
Abbreviations: CIN, cumulative incidence; E., Echinococcus; N/A, not applicable Footnotes
|
|||
The Territories region had the absolute highest mean annual CIN of echinococcosis cases overall, at 6.2 cases per million (Table 2). Though case counts were low, over the two decades, there was an increase in the Northwest Territories (6.3–9.1 cases per million) but decreases in Nunavut (8.6–2.6 cases per million) and Yukon (5.3–5.1 cases per million) (Figure 2), resulting in a regional absolute decrease in mean annual CIN from 6.8 to 5.6 cases per million.
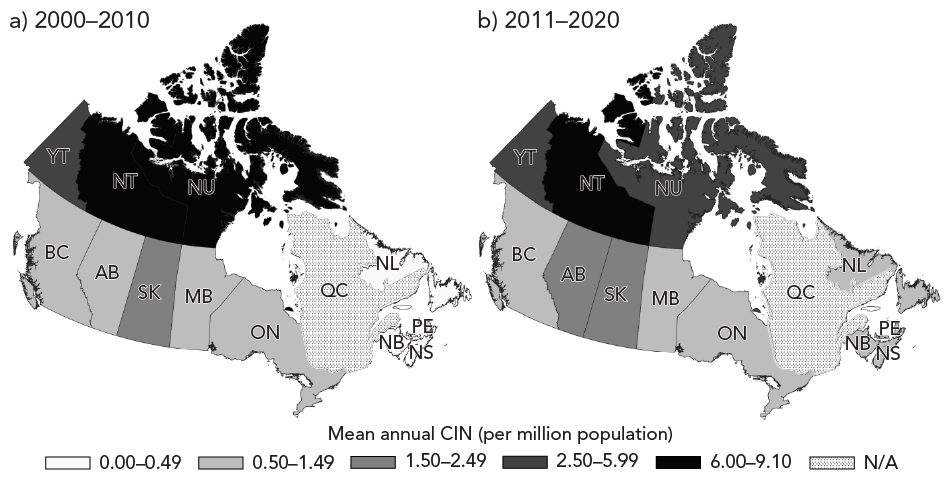
Figure 2 - Text description
| Geography | Mean annual cumulative incidence of echinococcosis cases (per million) |
Echinococcosis cases | Province or territory unique identifier (PRUID) |
|---|---|---|---|
| 2000–2010 | |||
| Alberta | 1.486077095 | 55 | 48 |
| British Columbia | 1.383189164 | 64 | 59 |
| Manitoba | 1.3761923 | 18 | 46 |
| New Brunswick | 0.364059914 | 3 | 13 |
| Newfoundland and Labrador | 0.353328681 | 2 | 10 |
| Nova Scotia | 0.09683645 | 1 | 12 |
| Northwest Territories | 6.281754833 | 3 | 61 |
| Nunavut | 8.641830381 | 3 | 62 |
| Ontario | 1.37826679 | 191 | 35 |
| Prince Edward Island | 0 | 0 | 11 |
| Saskatchewan | 1.980741081 | 22 | 47 |
| Yukon | 5.342667122 | 2 | 60 |
| Québec | N/A | 65 | 24 |
| 2011–2020 | |||
| Alberta | 2.405838173 | 100 | 48 |
| British Columbia | 0.779913111 | 38 | 59 |
| Manitoba | 1.462085144 | 19 | 46 |
| New Brunswick | 0.518231442 | 4 | 13 |
| Newfoundland and Labrador | 0.568729044 | 3 | 10 |
| Nova Scotia | 0.5275066 | 5 | 12 |
| Northwest Territories | 9.081012751 | 4 | 61 |
| Nunavut | 2.588996764 | 1 | 62 |
| Ontario | 1.290260501 | 180 | 35 |
| Prince Edward Island | 0.629810175 | 1 | 11 |
| Saskatchewan | 1.78097922 | 20 | 47 |
| Yukon | 5.144710449 | 2 | 60 |
| Québec | N/A | N/A | 24 |
Abbreviations: CIN, cumulative incidence; N/A, not applicable because Québec was excluded due to unavailable data between 2011–2020
- Footnote a
-
Including the Discharge Abstract Database (2000–2020), Hospital Morbidity Database (2000–2010) and National Ambulatory Care Reporting System (2003–2020)
Among provinces, the Western region had the absolute highest mean annual CIN of echinococcosis cases, at 1.6 cases per million (Table 2). In Alberta, the mean annual CIN increased over the two decades from 1.5 to 2.4 cases per million (Figure 2). The Eastern region, which only included Ontario due to limited data from Québec, had the second absolute highest mean annual CIN of echinococcosis cases overall, at 1.3 cases per million. In the Atlantic region, the mean annual CIN was low overall at 0.4 cases per million. However, though case counts were low, each province in the Atlantic region experienced an increase in the mean annual CIN of cases over the two decades, resulting in a regional absolute increase from 0.2 to 0.6 cases per million.
Discussion
This study used administrative data to describe echinococcosis incidence and risk in Canada between 2000–2020. The mean annual CIN of echinococcosis in Canada over the study period was rare at 1.3 cases per million, which was slightly lower than the 1.5 cases per million reported by the European Surveillance System in 2020Footnote 20. Between 2001–2005 in Canada, Gilbert et al.Footnote 21 found a lower mean incidence than this study, at 0.72 echinococcosis hospitalizations per million. Schurer et al.Footnote 22 found a median annual incidence between 2002–2011 of 1.4 echinococcosis hospital and ambulatory visits per million. The Gilbert et al.Footnote 21 estimate may be lower because they only used HMDB and restricted to cases with only a first or second discharge diagnosis of echinococcosis. Schurer et al.Footnote 22 used the DAD and NACRS and included cases with an echinococcosis diagnosis in any of the 25 available discharge diagnoses. This study's use of the DAD, HMDB and NACRS may have been beneficial for capturing hospital and ambulatory visits more completely.
The results indicated an absolute increase, though small, in the mean annual CIN of echinococcosis cases in Canada between 2011–2020 compared to 2000–2010. Whether this was due to the European-type E. multilocularis strain first detected in Canada in 2009 remains unclear, as the species-level diagnosis for most cases was unspecified. Distinguishing E. multilocularis from E. granulosus in humans is not only an epidemiological but also a clinical necessity, as there are differences in prognosis, treatment, intermediate hosts and regional prevalenceFootnote 1. Species-level diagnosis is complex, involving imaging, microscopy and serologyFootnote 1. Serology is required for early stages of infection, while later stages may be diagnosed through histopathologyFootnote 23. For people in Canada, confirmatory diagnosis of E. multilocularis demonstrating larval tapeworms in histopathology samples can require species-specific polymerase chain reaction (PCR) or serologic testing in some provincesFootnote 24. While this PCR is done at a limited number of laboratories across North America, approved serologic testing is only performed at the Institute of Parasitology in SwitzerlandFootnote 23. Studies have recommended that accessible and standardized testing optimized for circulating species of Echinococcus and increased awareness of clinical signs among physicians and veterinarians in endemic regions, would help improve prognosis and surveillance in CanadaFootnote 12Footnote 22.
Over the two decades, there was a notable absolute increase in mean annual CIN of echinococcosis cases in the Northwest Territories. Having a health card from any of the three Territories also posed the highest risk of echinococcosis. The overall mean annual CIN for the Territories region (6.2 cases per million) was closer to that which has been recorded in European countries considered endemic for echinococcosis, like Luxembourg (4.8 cases per million)Footnote 20Footnote 25. Northern parts of Canada may be at higher risk of echinococcosis due to some populations hunting, consuming untreated surface water, keeping dogs as pets and working animals and harvesting potentially contaminated foodFootnote 5Footnote 21Footnote 22.
There was also an absolute increase in the mean annual CIN of echinococcosis cases in Alberta over the two decades. Alberta had the second-highest number of cases diagnosed as E. multilocularis following Ontario despite having a substantially smaller population. Between 2013–2020, 17 cases of human AE were identified in Alberta, all likely locally acquired and all five of the cases with molecular typing results showing presence of the European-type strainFootnote 13. Among coyotes in urban areas of Alberta, studies have highlighted an increasing prevalence of E. multilocularis, ranging from 25% between 2009–2011Footnote 26 to 65% between 2016–2018Footnote 8, with histology results from the region often confirming the presence of the European-type strainFootnote 9Footnote 27.
The Atlantic region had the lowest mean annual CIN of echinococcosis cases, but it increased slightly over the two decades. In the past 30 to 40 years, coyotes have reportedly expanded their range from the Great Lakes region of southern Canada into eastern CanadaFootnote 28. A recent study recorded the first ever instances of E. canadensis, a subtype of E. granulosus, in free-ranging wildlife in Atlantic Canada (one coyote and four moose), suggesting that coyote natural range expansion has a role in enabling the lifecycle of Echinococcus tapeworms in the regionFootnote 28.
Similar to previous Canadian literature, females in this study had a significantly higher risk of echinococcosis compared to males, warranting further investigationFootnote 21Footnote 22. Older age was also associated with a significantly higher risk of echinococcosis; however, this may be due to the long incubation period preceding clinical manifestations of the diseaseFootnote 1.
In the absence of national reporting and surveillance of echinococcosis in Canada, CIHI databases were explored as an option for monitoring cases of this potentially increasing zoonosis. Administrative data are useful for investigating disease epidemiology, as they are population-based, timely, accessible, provide large sample sizes and have broad jurisdictional coverage. However, administrative data are not collected for research purposes and may have quality and reliability issuesFootnote 29. There is value in prioritizing future studies to examine the validity of administrative data sources for studying zoonoses in the future.
Limitations
There are some limitations of this study. Though it was the only available nationwide data source for echinococcosis, using hospital and ambulatory data to estimate incidence likely resulted in an underestimation. Echinococcosis is rare with a long incubation period, increasing the chance of under or misdiagnosis and most, but not all, symptomatic infections require medical attentionFootnote 1. The incidence is also likely underestimated, both overall and for the Eastern region especially, because data for Québec were unavailable between 2011–2020 and Québec contributed 15% of all cases between 2000–2010.
Administrative data can have quality and reliability concerns and often lack information on potentially relevant indicators. For example, we did not have data on travel history and as echinococcosis has a long incubation period, this may have been relevant for understanding local disease acquisition. Additionally, not all P/Ts have mandated reporting to NACRS; those with mandated reporting may have contributed more echinococcosis cases than those without.
The RRs of echinococcosis for the Territories had wide CIs, likely because of small population sizes and indicate imprecision. Due to the small population sizes, the CIN for the Territories were also unstable.
Conclusion
This study fills an important gap by contributing a baseline for human echinococcosis in Canada between 2000–2020. Although echinococcosis is rare, there was a small absolute increase in the mean annual CIN of cases nationally between 2011–2020 compared to 2000–2010. Further research is needed to determine the role of the new European-type E. multilocularis strain, in addition to climate change, urbanization and anthropogenic activity, on disease burden. Improved and complete data are needed to understand differences across provinces and territories, in order to inform engagement with and guidelines for, public health partners, key risk groups and the general public. Research investigating the validity of administrative data for zoonoses is also warranted.
Authors' statement
- AK — Conceptualization, methodology, formal analysis, writing–original draft, writing–review & editing
- PKM — Supervision, conceptualization, methodology, writing–review & editing
- DAJ — Validation, writing–review & editing
Competing interests
None.
Acknowledgements
The authors would like to thank the Public Health Agency of Canada's Joanne Tataryn and Jillian Blackmore for their methodological feedback and Julie Vachon, Peter Buck, Lesley Doering and Kerry Robinson for their review of the manuscript.
Funding
This work was supported by the Public Health Agency of Canada.
References
- Footnote 1
-
World Health Organization/World Organisation for Animal Health. WHO/OIE manual on echinococcosis in humans and animals: A public health problem of global concern. Paris, FR: WHO/OIE; 2001. [Accessed 2022 Oct 1]. https://www.who.int/publications/i/item/929044522X
- Footnote 2
-
Schmidberger J, Uhlenbruck J, Schlingeloff P, Maksimov P, Conraths FJ, Mayer B, Kratzer W. Dog ownership and risk for alveolar echinococcosis, Germany. Emerg Infect Dis 2022;28(8):1597–605. https://doi.org/10.3201/eid2808.212514
- Footnote 3
-
Hotez PJ. Neglected infections of poverty among the indigenous peoples of the arctic. PLoS Negl Trop Dis 2010;4(1):e606. https://doi.org/10.1371/journal.pntd.0000606
- Footnote 4
-
Jenkins EJ, Castrodale LJ, de Rosemond SJ, Dixon BR, Elmore SA, Gesy KM, Hoberg EP, Polley L, Schurer JM, Simard M, Thompson RC. Tradition and transition: parasitic zoonoses of people and animals in Alaska, northern Canada, and Greenland. Adv Parasitol 2013;82:33–204. https://doi.org/10.1016/B978-0-12-407706-5.00002-2
- Footnote 5
-
Davidson RK, Lavikainen A, Konyaev S, Schurer J, Miller AL, Oksanen A. Echinococcus across the north: current knowledge, future challenges. Food Waterborne Parasitol 2016;4:39–53. https://doi.org/10.1016/j.fawpar.2016.08.001
- Footnote 6
-
Santa MA, Umhang G, Klein C, Grant DM, Ruckstuhl KE, Musiani M. It's a small world for parasites: evidence supporting the North American invasion of European Echinococcus multilocularis. Proc Biol Sci 2023;290(1994):20230128. https://doi.org/10.1098/rspb.2023.0128
- Footnote 7
-
Peregrine AS, Jenkins EJ, Barnes B, Johnson S, Polley L, Barker IK, De Wolf B, Gottstein B. Alveolar hydatid disease (Echinococcus multilocularis) in the liver of a Canadian dog in British Columbia, a newly endemic region. Can Vet J 2012;53(8):870–4.
- Footnote 8
-
Luong LT, Chambers JL, Moizis A, Stock TM, St Clair CC. Helminth parasites and zoonotic risk associated with urban coyotes (Canis latrans) in Alberta, Canada. J Helminthol 2020;94:e25. https://doi.org/10.1017/S0022149X1800113X
- Footnote 9
-
Gesy K, Hill JE, Schwantje H, Liccioli S, Jenkins EJ. Establishment of a European-type strain of Echinococcus multilocularis in Canadian wildlife. Parasitology 2013;140(9):1133–7. https://doi.org/10.1017/S0031182013000607
- Footnote 10
-
Samuel WM, Ramalingam S, Carbyn LN. Helminths in coyotes (Canis latrans Say), wolves (Canis lupus L.), and red foxes (Vulpes vulpes L.) of southwestern Manitoba. Can J Zool 1978;56(12):2614–7. https://doi.org/10.1139/z78-351
- Footnote 11
-
Kotwa JD, Isaksson M, Jardine CM, Campbell GD, Berke O, Pearl DL, Mercer NJ, Osterman-Lind E, Peregrine AS. Echinococcus multilocularis Infection, Southern Ontario, Canada. Emerg Infect Dis 2019;25(2):265–72. https://doi.org/10.3201/eid2502.180299
- Footnote 12
-
Massolo A, Liccioli S, Budke C, Klein C. Echinococcus multilocularis in North America: the great unknown. Parasite 2014;21:73. https://doi.org/10.1051/parasite/2014069
- Footnote 13
-
Houston S, Belga S, Buttenschoen K, Cooper R, Girgis S, Gottstein B, Low G, Massolo A, MacDonald C, Müller N, Preiksaitis J, Sarlieve P, Vaughan S, Kowalewska-Grochowska K. Epidemiological and clinical characteristics of alveolar echinococcosis: an emerging infectious disease in Alberta, Canada. Am J Trop Med Hyg 2021;104(5):1863–9. https://doi.org/10.4269/ajtmh.20-1577
- Footnote 14
-
Public Health Agency of Canada. Case definitions: Nationally notifiable diseases. Ottawa, ON: PHAC; 2022. [Accessed 2022 Oct 1]. https://diseases.canada.ca/notifiable/diseases-list
- Footnote 15
-
Canadian Institute for Health Information. Data holdings. Toronto, ON: CIHI; 2022. [Accessed 2022 May 1]. https://www.cihi.ca/en/access-data-and-reports/data-holdings
- Footnote 16
-
World Health Organization. International Classification of Diseases Manual of the international statistical classification of diseases, injuries, and causes of death. 9th revision, 1975 edition. Geneva, CH: WHO; 1977.
- Footnote 17
-
World Health Organization. International Classification of Diseases Manual of the international statistical classification of diseases and related health problems. 10th revision, 2016 edition. Geneva, CH: WHO; 2015.
- Footnote 18
-
Statistics Canada. 2011 Census of Population. Ottawa, ON: StatCan; 2011. [Accessed 2022 May 1]. https://www12.statcan.gc.ca/census-recensement/2011/dp-pd/index-eng.cfm
- Footnote 19
-
Statistics Canada. Population estimates, quarterly. Ottawa, ON: StatCan; 2022. [Accessed 2022 May 1]. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000901
- Footnote 20
-
European Centre for Disease Prevention and Control. Echinococcosis - Annual Epidemiological Report for 2020-2022. Solna, SE: ECDC; 2022. [Accessed 2022 Oct 1]. https://www.ecdc.europa.eu/en/publications-data/echinococcosis-annual-epidemiological-report-2020
- Footnote 21
-
Gilbert NL, Dare OK, Libman MD, Muchaal PK, Ogden NH. Hospitalization for trichinellosis and echinococcosis in Canada, 2001-2005: the tip of the iceberg? Can J Public Health 2010;101(4):337–40. https://doi.org/10.1007/BF03405298
- Footnote 22
-
Schurer JM, Rafferty E, Farag M, Zeng W, Jenkins EJ. Echinococcosis: An Economic Evaluation of a Veterinary Public Health Intervention in Rural Canada. PLoS Negl Trop Dis 2015;9(7):e0003883. https://doi.org/10.1371/journal.pntd.0003883
- Footnote 23
-
Public Health Ontario. Ontario public health standards: Requirements for programs, services, and accountability. Disease: Echinococcus multilocularis infection. Toronto, ON: PHO; 2022. [Accessed 2022 Oct 1]. https://files.ontario.ca/moh-ophs-echinococcus-multilocularis-infection-en-2022.pdf
- Footnote 24
-
Alberta Health. Alberta Public Health Disease Management Guidelines - Echinococcosis (Alveolar). Edmonton, AB: Alberta Health; 2022. [Accessed 2022 Oct 1]. https://open.alberta.ca/dataset/140a7c4a-d7bd-4909-b02f-24c7b35afc63/resource/65528d86-2571-42cd-a821-f4f93cbfaa9d/download/health-phdmg-echinococcus-2021-11.pdf
- Footnote 25
-
Martini M, Dumendiak S, Gagliardo A, Ragazzini F, La Rosa L, Giunchi D, Thielen F, Romig T, Massolo A, Wassermann M. Echinococcus multilocularis and other taeniid metacestodes of muskrats in Luxembourg: Prevalence, risk factors, parasite reproduction, and genetic diversity. Pathogens 2022;11(12):1414. https://doi.org/10.3390/pathogens11121414
- Footnote 26
-
Catalano S, Lejeune M, Liccioli S, Verocai GG, Gesy KM, Jenkins EJ, Kutz SJ, Fuentealba C, Duignan PJ, Massolo A. Echinococcus multilocularis in urban coyotes, Alberta, Canada. Emerg Infect Dis 2012;18(10):1625–8. https://doi.org/10.3201/eid1810.120119
- Footnote 27
-
Kolapo TU, Hay A, Gesy KM, Frey CF, Rothenburger JL, Joffe DJ. Canine alveolar echinococcosis: an emerging and costly introduced problem in North America. Transbound Emerg Dis 2023;2023:1. https://doi.org/10.1155/2023/5224160
- Footnote 28
-
Priest JM, McRuer DL, Stewart DT, Boudreau M, Power JW, Conboy G, Jenkins EJ, Kolapo TU, Shutler D. New geographic records for Echinococcus canadensis in coyotes and moose from Nova Scotia, Canada. Int J Parasitol Parasites Wildl 2021;16:285–8. https://doi.org/10.1016/j.ijppaw.2021.11.004
- Footnote 29
-
Butler AL, Smith M, Jones W, Adair CE, Vigod SN, Lesage A, Kurdyak P. Multi-province epidemiological research using linked administrative data: a case study from Canada. Int J Popul Data Sci 2018;3(3):443. https://doi.org/10.23889/ijpds.v3i3.443
Appendix
Supplemental material is available upon request to the author: ayisha.khalid@mail.utoronto.ca
Aggregated case count and incidence by Echinococcus species, geography and year

Page details
- Date modified: