
Invasive group iGAS surveillance in Island Health, British Columbia, 2022

 Download this article as a PDF
Download this article as a PDFPublished by: The Public Health Agency of Canada
Issue: Volume 49-7/8, July/August 2023: Enteric Diseases: A Major Health Problem in Canada
Date published: July/August 2023
ISSN: 1481-8531
Submit a manuscript
About CCDR
Browse
Volume 49-7/8, July/August 2023: Enteric Diseases: A Major Health Problem in Canada
Surveillance
Invasive group A streptococcal (iGAS) surveillance in Island Health, British Columbia, 2022
Andrea Nwosu1,2, Andrea Schut2, Christie Arlotti Wood2, Christine Urquhart2, Claudia Bachman2, Katelyn Thompson2, Julia Evans2, Kathleen Mills2, Lisa Wenstob2, Theresa Restemeyer2, Trista Galbraith2, Shannon Mason2, Stephanie Gabriel2, Twyla Gasper2, Cheryl Broeren2, Francine Lewis2, Dee Hoyano2, Sandra Allison2, Pamela Kibsey2, Angela Reid2, Maritia Gully2, Carl Swanson2
Affiliations
1 Canadian Field Epidemiology Training Program, Public Health Agency of Canada, Ottawa, ON
2 Island Health, Victoria, BC
Correspondence
Suggested citation
Nwosu A, Schut A, Arlotti Wood C, Urquhart C, Bachman C, Thompson K, Evans J, Mills K, Wenstob L, Restemeyer T, Galbraith T, Mason S, Gabriel S, Gasper T, Broeren C, Lewis F, Hoyano D, Allison S, Kibsey P, Reid A, Gully M, Swanson C. Invasive group A streptococcal (iGAS) surveillance in Island Health, British Columbia, 2022. Can Commun Dis Rep 2023;49(7/8):342–50. https://doi.org/10.14745/ccdr.v49i78a06
Keywords: iGAS, group A streptococcus, Streptococcus pyogenes, emm, surveillance, British Columbia, Canada
Abstract
Background: Invasive group A streptococcal disease (iGAS) is caused by Streptococcus pyogenes group A bacteria. In 2022, multiple disease alerts for iGAS in the Island Health region, in the context of increased infections in the paediatric population in Europe and the United States, prompted further investigation into local trends. This surveillance study summarizes epidemiological trends of iGAS in the region covered by Island Health, a regional health authority in British Columbia, in 2022.
Methods: In British Columbia, iGAS is a reportable disease; all confirmed cases are reported to the regional authority and the provincial health authority (BC Centre for Disease Control). Island Health’s iGAS surveillance system is passive and collects information on cases that are identified through laboratory testing. Surveillance data were summarized for 2022 and compared with historical data from 2017–2021.
Results: In 2022, the incidence rate was 11.4 cases per 100,000 population (n=101), the highest observed rate in the last six years. The median age of cases was 53 years, with a range of 0–96 years, and 64% of cases were male. The highest risk of infection was reported in men 40–59 years of age, with an incidence rate of 21.3 cases per 100,000 population. The most common emm types were emm92 (n=14), emm49 (n=13), and emm83 (n=12). Overall, 85% (n=86) of cases were hospitalized, 21% (n=21) were admitted to the intensive care unit, and 6% (n=6) died.
Conclusion: This study highlights that the incidence of iGAS in the Island Health region continued to increase throughout the coronavirus disease 2019 (COVID-19) pandemic, reaching its highest annual rate in 2022. In contrast to reports from Europe and the United States, there was no notable increase in infections in the paediatric population. Given the sustained increase in iGAS activity, continued monitoring and description of the epidemiology of these cases on a regular basis is imperative.
Introduction
Group A streptococcal disease (GAS) is caused by Streptococcus pyogenes group A bacteria Footnote 1. A GAS infection is considered invasive when bacteria is detected at a sterile site within the bodyFootnote 1. Invasive group A streptococcus (iGAS) causes severe and in some cases life-threatening illnessFootnote 1. In 2022, multiple disease alerts for iGAS in Island Health, a regional health authority in British Columbia, in the context of reports of increased infections in the pediatric population in Europe and the United States, prompted further investigation into local trendsFootnote 2Footnote 3. The following surveillance report summarizes epidemiological trends of iGAS in Island Health, British Columbia in 2022.
Methods
Population
Island Health is one of five regional health authorities in British Columbia. The Island Health region has a population of about 860,000 people, which includes residents of Vancouver Island, the Islands in the Salish Sea and the Johnstone Straight, and the mainland communities north of Powell River and south of Rivers Inlet (Figure 1)Footnote 4. The region is divided into three health service delivery areas (HSDAs): North, Central and South Island.
Figure 1: Island Health Region of British Columbia

Figure 1 - Text description
This figure is a map displaying the five regional health authorities of British Columbia and the three different health service delivery areas of Island Health.
Case definitions
Confirmed case
Laboratory confirmation of infection with or without clinical evidence of invasive disease: isolation of group A streptococcus (S. pyogenes) from a normally sterile site, or demonstration of S. pyogenes DNA by an appropriately validated nucleic acid test from a normally sterile siteFootnote 5.
Probable case
Clinical evidence of invasive disease in the absence of another identified etiology and with non-confirmatory laboratory evidence of infection: isolation of group A streptococcus from a non-sterile site, or positive group A streptococcus antigen detectionFootnote 5.
Surveillance methods
In British Columbia, iGAS is a reportable disease; all confirmed cases are reported to the regional health authority and then to the BC Centre for Disease Control (BCCDC). Island Health’s iGAS surveillance system is a passive case-based system that relies on the collection of information about cases that are identified through laboratory testing. Laboratory testing of iGAS is conducted locally at Island Health laboratories. Positive bacterial cultures are then sent to the BCCDC Public Health Laboratory for confirmatory testing. Subtyping (emm typing) of all isolates is conducted by the Canadian National Microbiology Laboratory (NML). Information on case demographics, clinical progression of illness, and risk factors are collected using a standardized surveillance form.
Island Health case-level data were extracted from BCCDC’s Public Health Reporting Data Warehouse on February 1, 2023, at 12:00 p.m. PST. The case line list included episode date and information on age, sex, risk factors, and outcomes. The episode date is equal to the onset date if available. If the onset date is not available, then the clinical diagnosis date is used, followed by the earliest of specimen collection date, laboratory result date, or report date.
Data analysis
All analyses were performed using R version 4.1.1 and RStudio version 1.4.1717. Trends in case counts, incidence rates, geographic distribution, demographics, severity, and risk factors were summarized for 2022 and compared with historical data from 2017–2021. Population denominators were used to calculate rates.
Results
Trends in case counts and rates
Incidence rates of iGAS in the Island Health region have been increasing since 2019 (Figure 2). From 2017 to 2022, incidence rates ranged from 6.7 cases to 11.4 cases per 100,000 population. In 2022, 101 confirmed cases of iGAS were reported in the Island Health region. The incidence rate was 11.4 cases per 100,000 population, which was above the preliminary annual provincial rate (8.5 cases per 100,000 population) and the highest observed incidence in the last six years.
Figure 2: Invasive group A streptococcal disease cases and incidence rates by year, Island Health, 2017–2022 (n=418)

Figure 2 - Text description
This figure is a bar and line graph displaying the count of invasive group A streptococcal disease (iGAS) cases (bar graph) and the incidence of iGAS cases per 100,000 population (line graph) in Island Health from 2017 to 2022, by year.
| Episode year | Confirmed cases | Incidence rate Island Health | Incidence rate BC |
|---|---|---|---|
2017 |
55 |
6.7 |
8.5 |
2018 |
72 |
8.6 |
8.2 |
2019 |
55 |
6.5 |
7.8 |
2020 |
65 |
7.6 |
6.9 |
2021 |
70 |
8.1 |
7.8 |
2022 |
101 |
11.4 |
8.5 |
The number of reported cases ranged from 3–15 cases per month (incidence range: 0.3 cases to 1.7 cases per 100,000 population) (Figure 3). The highest observed cases and monthly incidence rates were in January, November, and December (15 cases, incidence rate: 1.7 cases per 100,000 population). In January and November, the number of cases and incidence rate exceeded the maximum cases and incidence seen in the previous five years. The number of cases in these months were 2.5 times and 1.9 times the maximum number of cases reported in the previous five years.
Figure 3: Invasive group A streptococcal disease cases and incidence rates by month, Island Health, 2022 compared to 2017–2021
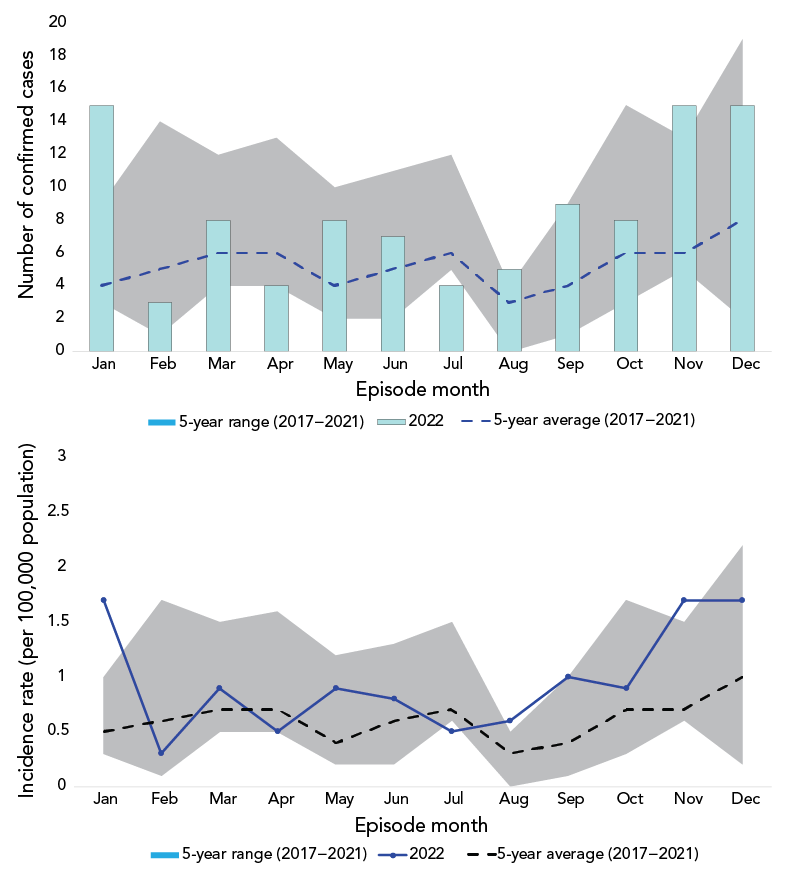
Figure 3 - Text description
This figure contains two graphs. The first graph is a bar and line graph comparing the count of invasive group A streptococcal disease (iGAS) cases in 2022 (bar graph) to the five-year (2017–2021) average number of iGAS cases (line graph) in Island Health by month. There is a shaded area on the graph displaying the five-year range for case counts. The second graph is a line graph comparing the incidence of iGAS cases per 100,000 population in 2022 to the five-year average incidence of iGAS cases per 100,000 in Island Health, by month. There is a shaded area on the graph displaying the five-year range for monthly incidence rates.
| Episode month | Confirmed cases | Incidence | ||||||
|---|---|---|---|---|---|---|---|---|
2022 |
5-year min |
5-year max |
5-year average |
2022 |
5-year min |
5-year max |
5-year average |
|
Jan |
15 |
3 |
6 |
4 |
1.7 |
0.3 |
0.7 |
0.5 |
Feb |
3 |
1 |
13 |
5 |
0.3 |
0.1 |
1.6 |
0.6 |
Mar |
8 |
4 |
8 |
6 |
0.9 |
0.5 |
1 |
0.7 |
Apr |
4 |
4 |
9 |
6 |
0.5 |
0.5 |
1.1 |
0.7 |
May |
8 |
2 |
8 |
4 |
0.9 |
0.2 |
1 |
0.4 |
Jun |
7 |
2 |
9 |
5 |
0.8 |
0.2 |
1.1 |
0.6 |
Jul |
4 |
5 |
7 |
6 |
0.5 |
0.6 |
0.9 |
0.7 |
Aug |
5 |
0 |
4 |
3 |
0.6 |
0 |
0.5 |
0.3 |
Sep |
9 |
1 |
8 |
4 |
1 |
0.1 |
0.9 |
0.4 |
Oct |
8 |
3 |
12 |
6 |
0.9 |
0.3 |
1.4 |
0.7 |
Nov |
15 |
5 |
8 |
6 |
1.7 |
0.6 |
0.9 |
0.7 |
Dec |
15 |
2 |
17 |
8 |
1.7 |
0.2 |
2 |
1 |
Geographic distribution
The incidence rates in 2022 ranged from 7.9 to 16.0 cases per 100,000 population in the three HSDAs (Figure 4). The incidence rates in both North and Central Island exceeded the rates for the entire Island Health Region. Since 2019, the incidence rates in Central Island have been increasing. In North Island, the incidence rates increased from 2019 to 2021 and decreased in 2022. In South Island, the incidence rates decreased from 2019 to 2021 and increased in 2022. In 2022, the highest incidence rate occurred in Central Island at 16.0 cases per 100,000 population. Forty-nine cases were reported from Central Island, which is an increase of 19 cases (63% increase) compared to the number reported in the previous year.
Figure 4: Invasive group A streptococcal disease incidence rates by health service delivery area and year, Island Health, 2017–2022
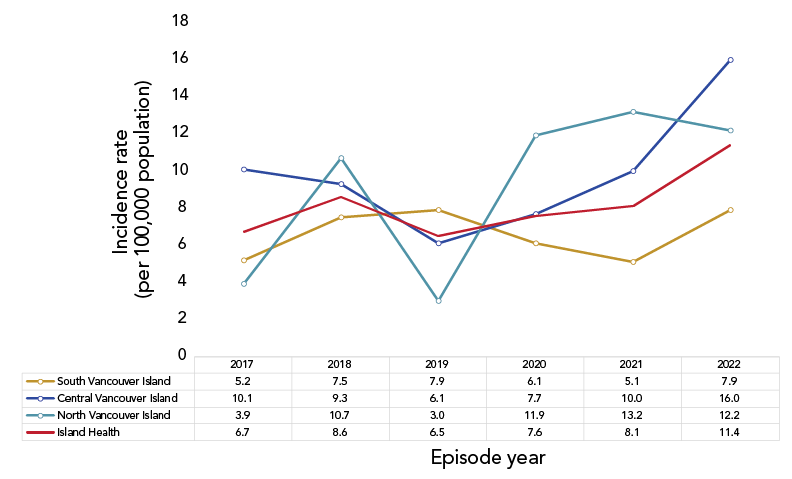
Figure 4 - Text description
This figure is a line graph displaying the incidence invasive group A streptococcal disease (iGAS) cases per 100,000 by year and by health service delivery area in Island Health from 2017 to 2022.
| Episode year | South Vancouver Island | Central Vancouver Island | North Vancouver Island | Island Health |
|---|---|---|---|---|
2017 |
5.2 |
10.1 |
3.9 |
6.7 |
2018 |
7.5 |
9.3 |
10.7 |
8.6 |
2019 |
7.9 |
6.1 |
3.0 |
6.5 |
2020 |
6.1 |
7.7 |
11.9 |
7.6 |
2021 |
5.1 |
10.0 |
13.2 |
8.1 |
2022 |
7.9 |
16.0 |
12.2 |
11.4 |
Demographic distribution
The median age of cases was 53 years, with a range of 0–96 years and 64% of cases were male. The distribution and risk of infection were the highest in men (distribution: 64%, incidence: 15.0 cases per 100,000 population) and individuals 40 years of age and older (distribution: 76%, incidence: 14.7 cases per 100,000 population) (Table 1). The highest incidence was reported in men 40–59 years of age (21.3 cases per 100,000 population) (Figure 5).
Demographics |
2022 | Average (2017–2021) | ||||
|---|---|---|---|---|---|---|
| Number of cases | Distribution | Incidence rate (per 100,000 population) |
Number of cases | Distribution | Incidence rate (per 100,000 population) |
|
Age group (years) |
||||||
0–4 |
2 |
2% |
6.1 |
1 |
2% |
4.1 |
5–9 |
2 |
2% |
5.1 |
0 |
1% |
1.1 |
10–19 |
1 |
1% |
1.2 |
2 |
3% |
2.1 |
20–39 |
20 |
20% |
9.3 |
13 |
21% |
6.4 |
40–59 |
35 |
35% |
15.8 |
22 |
34% |
9.9 |
60+ |
41 |
41% |
13.9 |
25 |
40% |
9.3 |
Sex |
||||||
Female |
36 |
36% |
8.0 |
25 |
40% |
5.9 |
Male |
65 |
64% |
15.0 |
38 |
60% |
9.2 |
Figure 5: Invasive group A streptococcal disease cases and incidence rates by age and sex, Island Health, 2022 compared to 2017–2021

Figure 5 - Text description
This figure is an age gender pyramid of the incidence rates of invasive group A streptococcal disease (iGAS) cases per 100,000 population in 2022.
| Age groups | 2022 | Average | ||
|---|---|---|---|---|
| Male incidence | Female incidence | Male incidence | Female incidence | |
60+ |
18.2 |
10.1 |
12.0 |
7.0 |
40–59 |
21.3 |
10.6 |
12.1 |
7.8 |
20–39 |
11.9 |
6.6 |
7.8 |
5.0 |
10–19 |
2.4 |
0.0 |
2.0 |
2.1 |
5–9 |
5.0 |
5.3 |
2.1 |
0.0 |
0–4 |
12.0 |
0.0 |
3.4 |
4.9 |
Emm typing
In 2022, there was no single dominant emm type. The three most common reported emm types were emm92 (n=14), emm49 (n=13), and emm83 (n=12) (Table 2).
| Emm type | 2017 |
2018 |
2019 |
2020 |
2021 |
Average (2017–2021) |
2022 |
|---|---|---|---|---|---|---|---|
emm92 |
1 |
0 |
0 |
0 |
8 |
2 |
|
emm49 |
0 |
0 |
0 |
1 |
3 |
||
emm83 |
0 |
2 |
4 |
4 |
2 |
2 |
|
emm74 |
0 |
0 |
1 |
0 |
1 |
0 |
9 |
emm59 |
0 |
0 |
0 |
5 |
6 |
2 |
8 |
emm43 |
0 |
0 |
0 |
0 |
2 |
0 |
6 |
emm76 |
1 |
2 |
5 |
1 |
5 |
4 |
|
emm53 |
3 |
3 |
4 |
4 |
1 |
3 |
3 |
emm12 |
0 |
1 |
0 |
1 |
0 |
0 |
3 |
emm11 |
1 |
0 |
1 |
0 |
2 |
1 |
2 |
emm77 |
4 |
0 |
3 |
2 |
4 |
3 |
2 |
emm82 |
2 |
1 |
1 |
1 |
2 |
2 |
|
emm1 |
3 |
11 |
6 |
1 |
0 |
4 |
1 |
emm101 |
2 |
2 |
3 |
3 |
3 |
1 |
|
emm22 |
1 |
0 |
0 |
0 |
0 |
0 |
1 |
emm41 |
4 |
1 |
8 |
1 |
|||
emm89 |
4 |
2 |
0 |
1 |
1 |
2 |
1 |
emm81 |
0 |
3 |
1 |
3 |
0 |
1 |
1 |
emm114 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
emm104 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
emm2 |
3 |
0 |
0 |
0 |
0 |
1 |
0 |
emm28 |
2 |
1 |
1 |
1 |
0 |
1 |
0 |
emm3 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
emm4 |
1 |
1 |
2 |
0 |
0 |
1 |
0 |
emm73 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
emm87 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
emm91 |
1 |
3 |
1 |
0 |
0 |
1 |
0 |
emm118 |
0 |
0 |
1 |
0 |
0 |
0 |
0 |
emm78 |
0 |
0 |
1 |
1 |
0 |
0 |
0 |
emm6 |
0 |
0 |
0 |
5 |
0 |
1 |
0 |
emm68 |
0 |
0 |
0 |
2 |
0 |
0 |
0 |
emm9 |
0 |
0 |
0 |
1 |
0 |
0 |
0 |
emm51 |
0 |
0 |
0 |
0 |
1 |
0 |
0 |
emm75 |
0 |
0 |
0 |
0 |
2 |
0 |
0 |
Unknown |
11 |
9 |
13 |
16 |
19 |
14 |
16 |
Severity
Twenty-seven percent of cases reported in 2022 were clinically classified as severe (Table 3). Severe cases are defined as cases of streptococcal toxic shock syndrome (STSS), soft-tissue necrosis (including necrotizing fasciitis, myositis, or gangrene), meningitis, GAS pneumonia, or death directly attributable to GAS infectionFootnote 6. Overall, 85% of cases were hospitalized, 21% were admitted to the intensive care unit (ICU), and 6% died (Table 4). The proportion of cases admitted to the hospital and ICU was below the average number admitted in the previous five years (hospitalizations: average=90%, range=85%–93%; ICU admissions: average=23%, range=15%–32%). The case fatality rate was the same as the average case fatality rate reported in the previous five years (average=6%, range=4%–8%). The deaths reported in 2022 occurred in men and women 52–89 years of age (median age=73 years, 67% female). All cases had multiple risk factors reported (median number of reported risk factors=4, range=2–5). Five different emm types were prevalent amongst these fatal cases: 74, 81, 83, 92, and 43.
| Severity | 2022 | Average (2017–2022) | ||
|---|---|---|---|---|
| Cases | Distribution | Cases | Distribution | |
Severe |
27 |
27% |
13 |
21% |
Non-severe |
74 |
73% |
38 |
60% |
Unknown |
0 |
0% |
12 |
19% |
| Outcomes | 2022 | Average (2017–2022) | ||
|---|---|---|---|---|
| Cases | Distribution | Cases | Distribution | |
Hospitalizations |
86 |
85% |
57 |
90% |
ICU admissions |
21 |
21% |
15 |
23% |
Deaths |
6 |
6% |
4 |
6% |
There was no dominant emm type reported among severe cases. For both severe and non-severe cases, the most common emm types were the same (Figure 6).
Figure 6: Distribution of streptococcal pyogenes emm types by severity, Island Health, 2022

Figure 6 - Text description
This figure is a bar graph showing the distribution of emm types by severity status in Island Health in 2022.
| Emm type | Severe | Non-severe |
|---|---|---|
emm92 |
7% |
16% |
emm49 |
11% |
14% |
emm83 |
7% |
14% |
emm74 |
7% |
9% |
emm59 |
7% |
8% |
Other |
41% |
24% |
Unknown |
19% |
15% |
Risk factors
The most common reported risk factors among cases were having a skin infection, 47% (n=47) and having a wound, 46% (n=46) (Table 5). Compared to the previous five years, skin infections, wounds, alcohol use disorder, unstable housing, chronic cardiac conditions, chronic respiratory conditions, and immunocompromised conditions were reported more frequently in 2022, while injection drug use was reported less frequently. Among severe cases (n=27), the most common reported risk factors were having a wound, 52% (n=14); using substances, 52% (n=14); or having a skin infection, 44% (n=12) (Table 6). For non-severe cases (n=74), the most common reported risk factors were having a skin infection, 47% (n=35) or having a wound, 43% (n=32).
| Risk factors | 2022 | Average (2017–2022) | ||
|---|---|---|---|---|
| Cases | Distribution | Cases | Distribution | |
Skin infection |
47 |
47% |
24 |
38% |
Wound |
46 |
46% |
22 |
34% |
Substance useFootnote a |
40 |
40% |
25 |
39% |
Chronic cardiac condition |
31 |
31% |
13 |
21% |
Homeless/underhoused |
27 |
27% |
14 |
23% |
Alcohol use disorder |
26 |
26% |
14 |
22% |
Chronic respiratory condition |
21 |
21% |
9 |
14% |
Diabetes |
19 |
19% |
11 |
17% |
Injection drug use |
17 |
17% |
14 |
22% |
Immunocompromised |
12 |
12% |
5 |
8% |
Substance use, otherFootnote b |
2 |
2% |
1 |
2% |
Tobacco use |
1 |
1% |
1 |
1% |
| Risk factors | Severe (n = 27) |
Non-severe (n = 74) |
|---|---|---|
Wound |
52% |
43% |
Substance useFootnote a |
52% |
35% |
Skin infection |
44% |
47% |
Chronic cardiac condition |
37% |
28% |
Alcohol use disorder |
37% |
22% |
Chronic respiratory condition |
30% |
18% |
Diabetes |
26% |
16% |
Homeless/underhoused |
26% |
27% |
Immunocompromised |
22% |
8% |
Injection drug use |
19% |
16% |
Tobacco use |
0% |
1% |
Substance use, otherFootnote b |
0% |
3% |
Discussion
In 2022, 101 confirmed cases of iGAS were reported in the Island Health region, corresponding to an incidence rate of 11.4 cases per 100,000 population; the highest rate reported in the last six years and above the preliminary annual provincial rate (8.5 cases per 100,000 population). Since 2019, the incidence of iGAS has been increasing in the Island Health region. This includes throughout the pandemic period when implemented non-pharmaceutical containment measures were also associated with a decrease in invasive respiratory diseases worldwideFootnote 7. Provincially, in British Columbia, rates of iGAS have been higher than expected since 2017, with the incidence in the last six years remaining stableFootnote 8. Globally, an increase in the incidence of iGAS over time has also been observed in many countries, including CanadaFootnote 9Footnote 10Footnote 11Footnote 12. Previous analyses have hypothesized that the observed increase is linked to both the increase in genetic diversity of circulating emm types and compounding societal risk factors, such as homelessness and substance useFootnote 10Footnote 13Footnote 14Footnote 15Footnote 16Footnote 17. Although the factors associated with the increased incidence seen in the Island Health region since 2019, and particularly in 2022, are not completely clear, it is likely that multiple factors have contributed to the observed trends. This includes increased circulation of respiratory viruses, an increase in the diversity in circulating emm types, and the impact of the coronavirus disease 2019 (COVID-19) pandemic on community services, specifically an increased demand paired with reduced capacity and availability.
In December 2022, several European countries and the United States reported recent increases in infections of iGAS in childrenFootnote 2Footnote 3. Similar to the provincial picture in British Columbia, demographic analysis of Island Health cases showed no notable increase in infections among the paediatric populationFootnote 8. The highest risk of infection was observed in men 40 years of age and older. While men 40 years of age and older appear to be at a higher risk for iGAS in 2022, further analysis on iGAS in this demographic group would contribute to understanding whether this is a confounding factor, since other risk factors, such as substance use, are known to be higher in this populationFootnote 18Footnote 19Footnote 20.
In 2022, no single dominant emm type was identified in the Island Health region. The three most common reported emm types were emm92 (n=14), emm49 (n=13), and emm83 (n=12). Prior to 2021, these emm types were uncommon in the Island Health region and British Columbia, representing on average 0.4%–4% and 1% of subtyped cases reported from 2016 to 2020, respectivelyFootnote 8. Nationally, emm1 has been the dominant emm type for the last decadeFootnote 21. Since 2014, the prevalence of emm1 has been decreasing nationally and was surpassed by emm76 in 2019 and emm49 in 2020Footnote 9Footnote 22Footnote 23Footnote 24. To date in the available literature, emm types 49, 83, and 92 have not been associated with more life-threatening illness. Emm types 1 and 3 have been associated with more life-threatening illness, but only represented 1% of cases subtyped in the Island Health region in 2022Footnote 25Footnote 26Footnote 27. Overall, indicators of severity in the Island Health region were either below the average or within range of the values reported in the previous five years.
Limitations
When breaking down case numbers by subgroups, cell sizes become small. Calculated rates where the numerator is less than 20 are unstable and should be interpreted with caution. The descriptive analyses where cases are broken down by month, by HSDA (applies to North Island), by age (applies to age categories younger than 20 years of age), and by age and sex are affected by small cell sizes. Fluctuations in these values may indicate random variation rather than significant change in the rate. As well, information on risk factors is predominantly collected through chart reviews. These reviews may not capture the full medical or social history of each case, therefore risk factors among iGAS cases may be under-reported. The regional data presented in this report have undergone data quality assessment by Island Health, but data reconciliation processes for the provincial data are underway for cases reported for 2019 through 2022. The provincial rates shown are based on preliminary numbers, and final numbers and rates for the province may change. Lastly, this report includes data from pandemic response years and an analysis on the impact of the response on the completeness and trends of respiratory surveillance data in the Island Health region has not yet been conducted. It is likely that due to the response, both burden of disease and data completeness decreased, therefore, observed trends during these years might have been higher than reported in this publication. This would affect the interpretation of observed trends in 2022 in comparison to the previous five years. Despite these limitations, this summary contributes descriptive epidemiology that is important for understanding iGAS in the Canadian context.
Conclusion
Overall, this surveillance study characterizes cases of iGAS in the Island Health region in 2022 and compares these cases to those reported over the last five years. The study highlights that incidence of iGAS in the Island Health region continued to increase throughout the COVID-19 pandemic, reaching its highest annual rate in 2022. In contrast to reports from Europe and the United States, there was no notable increase in infections in the paediatric population. The findings of this report contribute to the epidemiological characterization of iGAS in Canada. Given the continued local, provincial, and national increase in incidence of iGAS, it is imperative that the epidemiology of these cases continues to be monitored and described annually.
Authors’ statement
- AN — Formal analysis, data curation, visualization, writing–original draft, review and editing of final version
- AS — Data collection, writing–review and editing
- CAW — Data collection, writing–review and editing
- CU — Data collection, writing–review and editing
- CB — Data collection, writing–review and editing
- KT — Data collection, writing–review and editing
- JE — Data collection, writing–review and editing
- KM — Data collection, writing–review and editing
- LW — Data collection, writing–review and editing
- TR — Data collection, writing–review and editing
- TGalbraith — Data collection, writing–review and editing
- SM — Data collection, writing–review and editing
- SG — Data collection, writing–review and editing
- TGasper — Data collection, writing–review and editing
- CB — Data collection, resources, methodology, writing–review and editing
- FL — Data collection, resources, methodology, writing–review and editing
- DH — Resources, methodology, writing–review and editing
- SA — Resources, methodology, writing–review and editing
- PK — Data collection, resources, laboratory validation and methodology, writing–review and editing
- AR — Resources, methodology, supervision, writing–review and editing
- MG — Resources, methodology, supervision, writing–review and editing
- CS — Resources, writing–review and editing
Competing interests
None.
References
- Footnote 1
-
BC Centre for Disease Control (BCCDC). Streptococcal disease, invasive, Group A. [Accessed 2022 Dec 29]. http://www.bccdc.ca/health-info/diseases-conditions/streptococcal-disease-invasive-group-a
- Footnote 2
-
World Health Organization. Disease Outbreak News; Increased incidence of scarlet fever and invasive Group A Streptococcus infection - multi-country. Geneva (CH): WHO; 2022. [Accessed 2022 Dec 29]. https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON429
- Footnote 3
-
Centers for Disease Control and Prevention (CDC). Increase in Invasive Group Strep Infections, 2022. Atlanta, GA: CDC; 2022. [Accessed 2022 Dec 29]. https://www.cdc.gov/groupastrep/igas-infections-investigation.html
- Footnote 4
-
Island Health. About Us. [Accessed 2022 Dec 29]. https://www.islandhealth.ca/about-us#:~:text=Island%20Health%20provides%20health%20care,communities%20north%20of%20Powell%20River
- Footnote 5
-
BC Centre for Disease Control (BCCDC). Streptococcal Disease, invasive Group A Case Definition. [Accessed 2022 Dec 29]. http://www.bccdc.ca/health-professionals/clinical-resources/case-definitions/streptococcal-disease-invasive-group-a
- Footnote 6
-
BC Centre for Disease Control (BCCDC). Communicable Disease Control Manual. Chapter 1: Communicable Disease Control. [Accessed 2022 Dec 30]. http://www.bccdc.ca/resource-gallery/Documents/Guidelines%20and%20Forms/Guidelines%20and%20Manuals/Epid/CD%20Manual/Chapter%201%20-%20CDC/iGAS.pdf
- Footnote 7
-
Brueggemann AB, Jansen van Rensburg MJ, Shaw D, McCarthy ND, Jolley KA, Maiden MC, van der Linden MP, Amin-Chowdhury Z, Bennett DE, Borrow R, Brandileone MC, Broughton K, Campbell R, Cao B, Casanova C, Choi EH, Chu YW, Clark SA, Claus H, Coelho J, Corcoran M, Cottrell S, Cunney RJ, Dalby T, Davies H, de Gouveia L, Deghmane AE, Demczuk W, Desmet S, Drew RJ, du Plessis M, Erlendsdottir H, Fry NK, Fuursted K, Gray SJ, Henriques-Normark B, Hale T, Hilty M, Hoffmann S, Humphreys H, Ip M, Jacobsson S, Johnston J, Kozakova J, Kristinsson KG, Krizova P, Kuch A, Ladhani SN, Lâm TT, Lebedova V, Lindholm L, Litt DJ, Martin I, Martiny D, Mattheus W, McElligott M, Meehan M, Meiring S, Mölling P, Morfeldt E, Morgan J, Mulhall RM, Muñoz-Almagro C, Murdoch DR, Murphy J, Musilek M, Mzabi A, Perez-Argüello A, Perrin M, Perry M, Redin A, Roberts R, Roberts M, Rokney A, Ron M, Scott KJ, Sheppard CL, Siira L, Skoczyńska A, Sloan M, Slotved HC, Smith AJ, Song JY, Taha MK, Toropainen M, Tsang D, Vainio A, van Sorge NM, Varon E, Vlach J, Vogel U, Vohrnova S, von Gottberg A, Zanella RC, Zhou F. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries and territories in the Invasive Respiratory Infection Surveillance Initiative: a prospective analysis of surveillance data. Lancet Digit Health 2021;3(6):e360–70. https://doi.org/10.1016/S2589-7500(21)00077-7
- Footnote 8
-
BC Centre for Disease Control (BCCDC). Invasive Group A Streptococcal Disease (iGAS) in British Columbia. Preliminary 2022 Annual Summary (to December 13, 2022). [Accessed 2022 Dec 29]. http://www.bccdc.ca/Documents/iGAS%20Epidemiological%20Summary%2020221216%20FINAL.pdf
- Footnote 9
-
Golden AR, Griffith A, Demczuk WH, Tyrrell GJ, Kus JV, McGeer A, Domingo MC, Hoang L, Minion J, Van Caeseele P, Smadi H, Haldane D, Zahariadis G, Mead K, Steven L, Strudwick L, Li AY, Mulvey MR, Martin I. Invasive group A streptococcal disease surveillance in Canada, 2020. Can Commun Dis Rep 2022;48(9):407–14. https://doi.org/10.14745/ccdr.v48i09a05
- Footnote 10
-
Blagden S, Watts V, Verlander NQ, Pegorie M. Invasive group A streptococcal infections in North West England: epidemiology, risk factors and fatal infection. Public Health 2020;186:63–70. https://doi.org/10.1016/j.puhe.2020.06.007
- Footnote 11
-
Oliver J, Wilmot M, Strachan J, St George S, Lane CR, Ballard SA, Sait M, Gibney K, Howden BP, Williamson DA. Recent trends in invasive group A Streptococcus disease in Victoria. Commun Dis Intell (2018) 2019;43:43. https://doi.org/10.33321/cdi.2019.43.8
- Footnote 12
-
Centers for Disease Control and Prevention (CDC). Active Bacterial Core surveillance (ABCs) report, Emerging infections program network, group A streptococcus, 2019. Atlanta, GA: CDC; 2019. [Accessed 2022 Feb 08]. https://www.cdc.gov/abcs/downloads/GAS_Surveillance_Report_2019.pdf
- Footnote 13
-
Tyrrell GJ, Fathima S, Kakulphimp J, Bell C. Increasing rates of invasive group A streptococcal disease in Alberta, Canada; 2003–2017. Open Forum Infect Dis 2018;5(8):ofy177. https://doi.org/10.1093/ofid/ofy177
- Footnote 14
-
Dickson C, Pham MT, Nguyen V, Brubacher C, Silverman MS, Khaled K, Hovhannisyan G. Community outbreak of invasive group A streptococcus infection in Ontario, Canada. Can Commun Dis Rep 2018;44(7-8):182–8. https://doi.org/10.14745/ccdr.v44i78a06
- Footnote 15
-
Athey TB, Teatero S, Sieswerda LE, Gubbay JB, Marchand-Austin A, Li A, Wasserscheid J, Dewar K, McGeer A, Williams D, Fittipaldi N. High incidence of invasive group A Streptococcus disease caused by strains of uncommon emm types in Thunder Bay, Ontario, Canada. J Clin Microbiol 2016;54(1):83–92. https://doi.org/10.1128/JCM.02201-15
- Footnote 16
-
Avire NJ, Whiley H, Ross K. A Review of Streptococcus pyogenes: public health risk factors, prevention and control. Pathogens 2021;10(2):248. https://doi.org/10.3390/pathogens10020248
- Footnote 17
-
Valenciano SJ, Onukwube J, Spiller MW, Thomas A, Como-Sabetti K, Schaffner W, Farley M, Petit S, Watt JP, Spina N, Harrison LH, Alden NB, Torres S, Arvay ML, Beall B, Van Beneden CA. Invasive group A streptococcal infections among people who inject drugs and people experiencing homelessness in the United States, 2010–2017. Clin Infect Dis 2021;73(11):e3718–26. https://doi.org/10.1093/cid/ciaa787
- Footnote 18
-
Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, Judd LL, Goodwin FK. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA 1990;264(19):2511–8. https://doi.org/10.1001/jama.1990.03450190043026
- Footnote 19
-
Compton WM, Thomas YF, Stinson FS, Grant BF. Prevalence, correlates, disability, and comorbidity of DSM-IV drug abuse and dependence in the United States: results from the national epidemiologic survey on alcohol and related conditions. Arch Gen Psychiatry 2007;64(5):566–76. https://doi.org/10.1001/archpsyc.64.5.566
- Footnote 20
-
Rehm J, Shield KD. Global burden of disease and the impact of mental and addictive disorders. Curr Psychiatry Rep 2019;21(2):10. https://doi.org/10.1007/s11920-019-0997-0
- Footnote 21
-
Gherardi G, Vitali LA, Creti R. Prevalent emm types among invasive GAS in Europe and North America since year 2000. Front Public Health 2018;6:59. https://doi.org/10.3389/fpubh.2018.00059
- Footnote 22
-
Public Health Agency of Canada. National laboratory surveillance of invasive streptococcal disease in Canada - Annual Summary 2017. Ottawa, ON: PHAC; 2017. [Accessed 2022 Jan 05]. https://www.canada.ca/en/public-health/services/publications/drugs-health-products/national-laboratory-surveillance-invasive-streptococcal-disease-annual-summary-2017.html
- Footnote 23
-
Public Health Agency of Canada. National laboratory surveillance of invasive streptococcal disease in Canada - Annual Summary 2018. Ottawa, ON: PHAC; 2018. [Accessed 2022 Jan 05]. https://www.canada.ca/en/public-health/services/publications/drugs-health-products/national-laboratory-surveillance-invasive-streptococcal-disease-canada-annual-summary-2018.html
- Footnote 24
-
Public Health Agency of Canada. National laboratory surveillance of invasive streptococcal disease in Canada - Annual Summary 2019. Ottawa, ON: PHAC; 2019. [Accessed 2022 Jan 05]. https://www.canada.ca/en/public-health/services/publications/drugs-health-products/national-laboratory-surveillance-invasive-streptococcal-disease-canada-annual-summary-2019.html
- Footnote 25
-
Wong CJ, Stevens DL. Serious group a streptococcal infections. Med Clin North Am 2013;97(4):721–36. https://doi.org/10.1016/j.mcna.2013.03.003
- Footnote 26
-
Lamagni TL, Neal S, Keshishian C, Hope V, George R, Duckworth G, Vuopio-Varkila J, Efstratiou A. Epidemic of severe Streptococcus pyogenes infections in injecting drug users in the UK, 2003-2004. Clin Microbiol Infect 2008;14(11):1002–9. https://doi.org/10.1111/j.1469-0691.2008.02076.x
- Footnote 27
-
Nelson GE, Pondo T, Toews KA, Farley MM, Lindegren ML, Lynfield R, Aragon D, Zansky SM, Watt JP, Cieslak PR, Angeles K, Harrison LH, Petit S, Beall B, Van Beneden CA. Epidemiology of invasive group A streptococcal infections in the United States, 2005–2012. Clin Infect Dis 2016;63(4):478–86. https://doi.org/10.1093/cid/ciw248

Page details
- Date modified: