
Inequalities in health of racialized adults in Canada
Download in PDF format
(576 KB, 1 page)
Organization: Public Health Agency of Canada
Date published: 2022-07-07
Racism is a key determinant of health and well-being12. Racism influences access to health promoting resources. Populations who are racialized in relation to a "white" or non-racialized social group experience stressors including inter-personal and systemic discrimination throughout the life course2.
Here we describe a snapshot of social and health inequalities for racialized populations from diverse cultural and racial backgrounds.
Physical Health: Diabetes, Obesity, Self-rated Health
Compared to White adults, the prevalence of diabetes3 is:
- 2.3 times higher among South Asian adults
- 1.9 times higher among Black adults
- 1.8 times higher among Arab/West Asian adults
Per 100 people,
- 9 more South Asian adults
- 6 more Black adults
- 6 more Arab/West Asian adults
Report having diabetes, compared to White adults.
The inequalities are more pronounced among men.
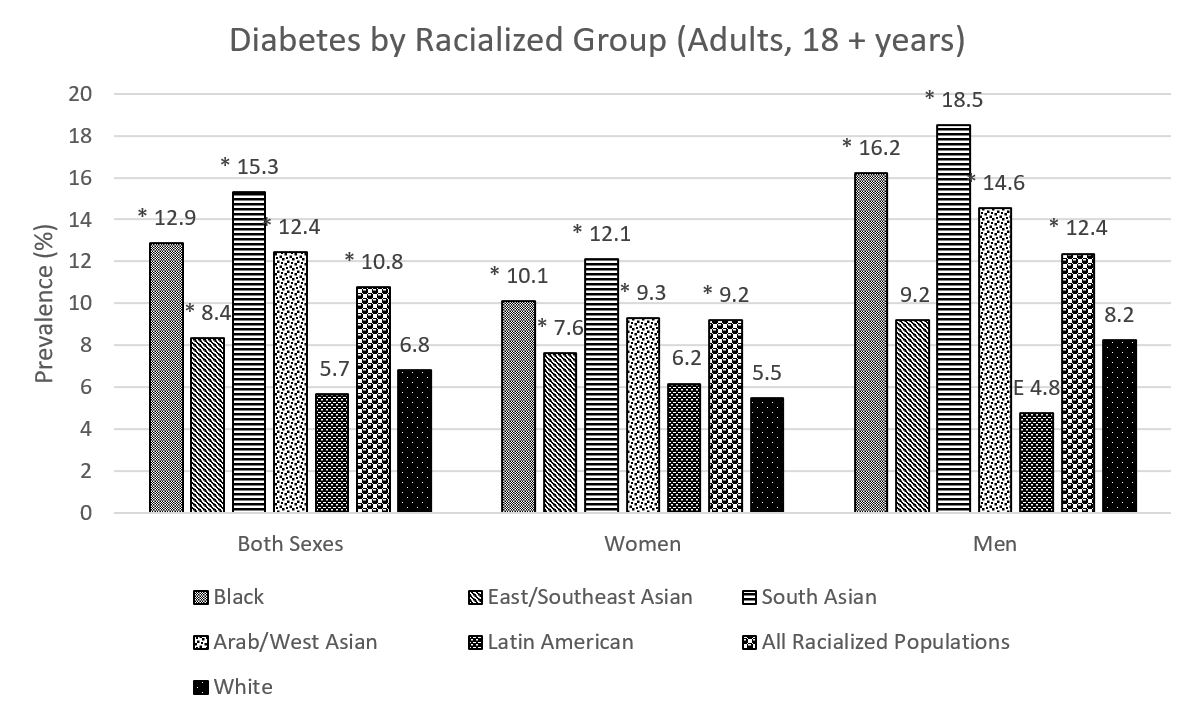
Table 1 – Prevalence (%) of Diabetes by Cultural/Racial Background and Sex/Gender (Adults, 18+ years)
| Cultural/Racial Background | Both Sexes | Women | Men |
| Black | 12.9* | 10.1* | 16.2* |
| East/Southeast Asian | 8.4* | 7.6* | 9.2 |
| South Asian | 15.3* | 12.1* | 18.5* |
| Arab/West Asian | 12.4* | 9.3* | 14.6* |
| Latin American | 5.7 | 6.2 | 4.8 E |
| All Racialized Populations | 10.8* | 9.2* | 12.4* |
| White | 6.8 | 5.5 | 8.2 |
*: Significantly different from reference category, by sex/gender groups
E: Interpret with caution
While most racialized adults are less likely to report a height and weight classified as obese, the proportion of obesity among Black women is 1.3 times that of white women.
Compared to White adults, racialized adults are less likely to feel that their health is either good or excellent. These inequalities are largest for women.
Per 100 women,
- 17 fewer Arab/West Asian women
- 12 fewer South Asian women
- 10 fewer East Asian/Southeast Asian women
- 8 fewer Black women
- 8 fewer Latin American women
feel very positively about their health, compared to white women.
Mental Health and Well-being: Self-rated Mental Health, Work Stress, Life Satisfaction
Across Canada, racialized communities typically experience higher exposure to life stressors45 ; however, mental health inequalities may appear smaller in these communities. This may be due to different cultural perceptions of mental health, experiences of stigma, and barriers to mental health services.46
East/Southeast Asian and Arab/West Asian adults are less likely to report that their mental health is excellent or good, compared to White adults.

Table 2 – Prevalence (%) of Perceived Excellent/Good Mental Health by Cultural/Racial Background (Adults, 18+ years)
| Cultural/Racial Background | Both Sexes |
| Black | 72.9 |
| East/Southeast Asian | 66.5* |
| South Asian | 70.0 |
| Arab/West Asian | 65.8* |
| Latin American | 70.0 |
| All Racialized Populations | 68.4* |
| White | 70.6 |
*: Significantly different from reference category
While most racialized adults are less likely to perceive their work stress as quite a bit or extremely stressful, Black and Arab/West Asian men are 1.2 times more likely to report feeling this way compared to White men.
Compared to White adults, there are 8 fewer Arab/West Asian adults, per 100 people, who report feeling satisfied or very satisfied with their lives.

Table 3 – Prevalence (%) of Average to High Life Satisfaction by Cultural/Racial Background and Sex/Gender (Adults, 18+ years)
| Cultural/Racial Background | Both Sexes | Women | Men |
| Black | 90.5* | 91.3 | 89.7* |
| East/Southeast Asian | 92.7 | 93.4 | 92.0 |
| South Asian | 90.5* | 91.3 | 89.7* |
| Arab/West Asian | 84.8* | 86.1* | 84.1* |
| Latin American | 94.2 | 92.7 | 96.0* |
| All Racialized Populations | 91.2* | 91.6* | 90.7* |
| White | 93.2 | 93.0 | 93.4 |
*: Significantly different from reference category, by sex/gender groups
Social Determinants and Health Behaviours
For racialized adults, inequalities exist in social determinants of health such as food security, housing, and access to health services.
Food Security
The prevalence of food insecurity among Black adults is the highest across all racialized groups, with a rate 2.8 times higher than White adults. This represents 13 more Black adults experiencing food insecurity per 100 people.
These inequalities are more pronounced among women, with Black women representing the highest proportion of adults experiencing food insecurity.

Table 4 – Prevalence (%) of Moderate to Severe Food Insecurity by Cultural/Racial Background and Sex/Gender (Adults, 18+ years)
| Cultural/Racial Background | Both Sexes | Women | Men |
| Black | 19.6* | 22.8* | 15.9* |
| East/Southeast Asian | 5.6* | 6.0* | 5.0 |
| South Asian | 7.7 | 6.6 E | 8.7* |
| Arab/West Asian | 13.3* | 13.3* | 12.8* |
| Latin American | 14.3* | 15.9* | 13.1* |
| All Racialized Populations | 9.1* | 9.9* | 8.2* |
| White | 6.9 | 8.1 | 5.7 |
*: Significantly different from reference category, by sex/gender groups.
E: Interpret with caution
Housing
Racialized Canadians are disproportionately impacted by inequalities in safe and stable housing. Arab/West Asian and Black Canadians are the most affected.
Compared to White Canadians, the proportion of those in core housing need7 is
- 2.7 times higher among Arab/West Asian Canadians
- 2.2 times higher among Black Canadians
- 2.0 times higher among East/Southeast Asian Canadians
- 1.9 times higher among Latin American Canadians
- 1.8 times higher among South Asian Canadians
Compared to White adults, the proportion of those who experienced major neighbourhood concerns 8 is:
- 1.6 higher among Arab/West Asian adults
- 1.5 higher among Black adults
Black adults are also 2.1 times more likely than White adults to have ever experienced homelessness.
Health Service Access
Compared to White adults, there are large inequalities in racialized adults' contact with dental professionals and regular health care providers.
- 13 fewer Arab/West Asian adults
- 10 fewer South Asian adults
- 9 fewer Black adults
Per 100 people, have contact with a dental professional (past year).
- 8 fewer Arab/West Asian adults
- 6 fewer Black adults
Per 100 people, have a regular health care provider (past year)
The lowest rates are among Arab/West Asian women where there are 7 fewer adults, per 100 people, who have a regular health care provider.
For more data on health inequalities in Canada, visit: https://health-infobase.canada.ca/health-inequalities/data-tool/Index
Notes: Rates presented in this infographic are age-standardized based on the 2016 Canadian population.
No data were available among people who identify as Non-binary, as information on gender was not collected prior in CCHS 2015-2018. For more information, visit: https://www150.statcan.gc.ca/n1/en/catalogue/982000012021001.
CHS collects gender information: male, female and other. Only the data for "Other" category is suppressed due to small numbers. The stratifier "All Racialized Populations" does not include First Nations, Inuit and Métis peoples.
- Footnote 1
-
Public Health Agency of Canada. (2020, September 8). Social Determinants and Inequities in Health for Black Canadians: A Snapshot. Canada.ca. Retrieved April 22, 2022, from https://www.canada.ca/en/public-health/services/health-promotion/population-health/what-determines-health/social-determinants-inequities-black-canadians-snapshot.html
- Footnote 2
-
National Collaborating Centre for Determinants of Health. (2018). Let's Talk: Racism and Health Equity (Rev. ed.). Antigonish, NS: National Collaborating Centre for Determinants of Health, St. Francis Xavier University.
- Footnote 3
-
Type 1 or 2 self-reported diabetes combined, excluding gestational.
- Footnote 4
-
Grace, S.L., Tan, Y., Cribbie, R.A. et al. The mental health status of ethnocultural minorities in Ontario and their mental health care. BMC Psychiatry 16, 47 (2016). https://doi.org/10.1186/s12888-016-0759-z
- Footnote 5
-
Public Health Agency of Canada, & Pan-Canadian Public Health Network. (2018, May 28). Government of Canada. Canada.ca. Retrieved from https://www.canada.ca/en/public-health/services/publications/science-research-data/key-health-inequalities-canada-national-portrait-executive-summary.html
- Footnote 6
-
Chiu, M., Amartey, A., Wang, X., & Kurdyak, P. (2018). Ethnic differences in mental health status and service utilization: A population-based study in Ontario, Canada. The Canadian Journal of Psychiatry, 63(7), 481–491. https://doi.org/10.1177/0706743717741061
- Footnote 7
-
Living in core housing need: 1) A household that does not meet one or more of the following: suitability, adequacy, and affordability standards; and 2) 30% or more of the household income (before-tax) would be necessary to acquire adequate housing that meets the three standards
https://www.cmhc-schl.gc.ca/en/professionals/housing-markets-data-and-research/housing-research/core-housing-need/identifying-core-housing-need - Footnote 8
-
Big neighbourhood issue: Noisy neighbours or loud parties, people hanging around the streets, garbage or litter lying around, vandalism/graffiti/other damage, attacks motivated by race/ethnicity/religion, people using or dealing drugs, people being drunk or rowdy in public, abandoned buildings, smog or air pollution https://www23.statcan.gc.ca/imdb/p3Instr.pl?Function=assembleInstr&lang=en&Item_Id=1291909#qb1294199
Sources: Canadian Community Health Survey (CCHS), 2015-16, 2017-18; Canadian Housing Survey, 2018
Page details
- Date modified: